
Although OSHA had not waived compliance with any of its requirements during the pandemic, the agency set forth temporary enforcement discretion policies that CSHOs could consider when enforcing OSHA standards, such as the Respiratory Protection standard, 29 CFR § 1910.134, and/or equivalent respiratory protection provisions of other health standards.
https://www.osha.gov/laws-regs/standardinterpretations/2021-07-07#:~:text=Although%20OSHA%20had,other%20health%20standards.
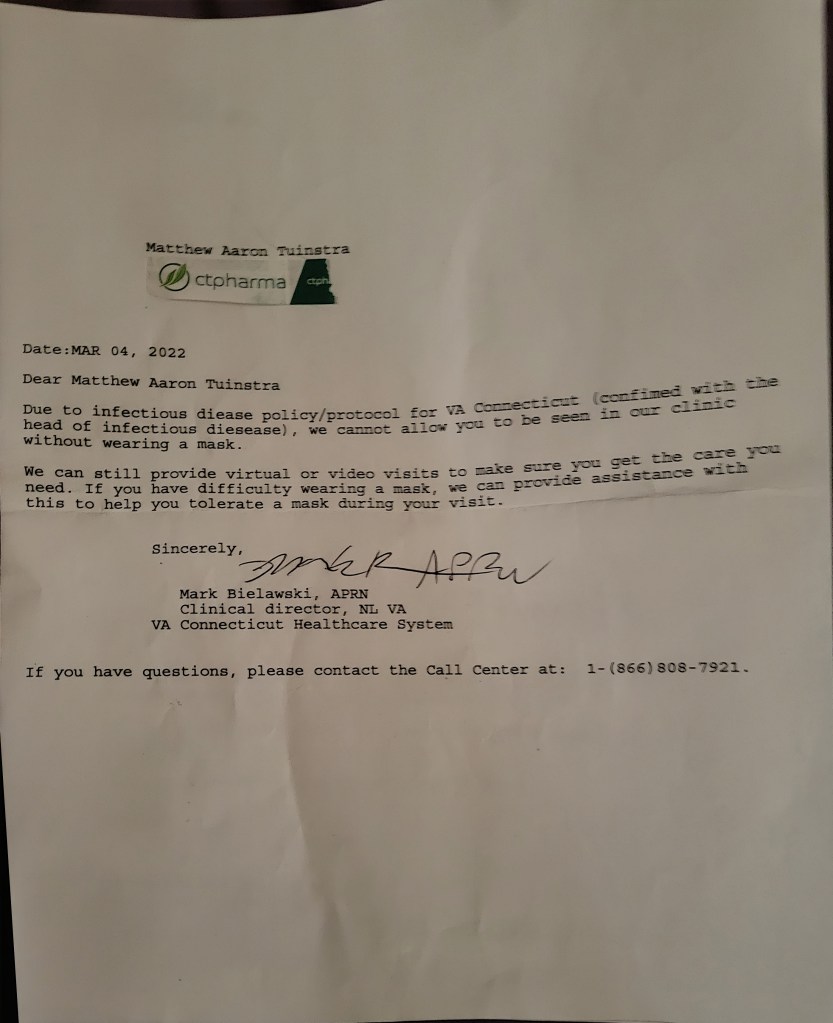
On Dec 2nd 2021 I was refused Medical treatment via Veterans Affairs. At this point in Time it had been 2 weeks since the Veterans Affairs Commissioner reported any positive results of SARS-COV, the total who did test positive was 76 Staff and 74 patrons where 5 patrons died with 2 staff members. I have been keeping track.

I made a Whistleblower claim to the Veterans Whistleblower online to report the “1910.134(d)(1)(ii)
The employer shall select a NIOSH-certified respirator. The respirator shall be used in compliance with the conditions of its certification” via Whistleblower Protection (OAWP) on 3/11/2022. Before that I reported the VA wearing the wrong masks in Dec 2021 after being refused medical treatment, only for Sam Glover from PA to refuse it, when clearly it was a violation, Sam Glover refused to take my claim. case referral 22-NorwichCT-18500. Other numbers
22-WestHavenCT-18503
22-WestHavenCT-18926
Here is another Veterans Affairs doing the same thing at Gilbert, Arizona on 7/20/2021 for 1910.134(d)(1)(ii) https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(d)(1)(ii,conditions%20of%20its%20certification
In 2019 OSHA 1910.134 was 4 on the top most reported violations, in 2020 it rose to 3ed after being 4th for decades, and in 2021 it jumped ro 2nd. So after the pandemic we started breaking the rules.
[OSHA inspections FY 2019 total federal inspections: 33,393](https://www.osha.gov/data/commonstats)
Here is a list off all Veterans Affairs 5A1 Citations (OSHA VIOLATIONS) https://www.osha.gov/enforcement/covid-19-data/inspections-covid-related-citations
Denver, Colorado 1/26/2021
1910.134(f)(2)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(f)(2,least%20annually%20thereafter
North Los Vagas, Nevada 4/27/2021
Salt Lake City, Utah 5/20/2021
1910.134(e)(1)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(e)(1),required%20to%20use%20a%20respirator
1910.134(e)(6)(i)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(e)(6)(i,only%20the%20following%20information
Gilbert, Arizona 7/20/2021
1910.134(d)(1)(ii)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(d)(1)(ii,conditions%20of%20its%20certification
1910.134(e)(6)(i)(A)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(e)(6)(i)(A,able%20to%20use%20the%20respirator%3B
1910.134(g)(1)(ii)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(g)(1)(ii,face%20of%20the%20user
Tucson, Arizona 10/26/2021
1910.502(l)(3)(i)(A)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(l)(3)(i)(A,date(s)%20that%20contact%20occurred
1910.502(l)(3)(i)(B)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(l)(3)(i)(B),workplace%20during%20the%20potential%20transmission%20period
1910.502(r)(ii)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(r)(2,and%20(b)(6)
1910.502(j)(2)(i)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(j)(2)(i,application%20of%20cleaners%3B%20and
Salisbury, South Carolina 12/02/2021
1910.502(h)(1)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(h)(1,hallways%20or%20aisles
1910.502(l)(3)(i)(B)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(l)(3)(i)(B),workplace%20during%20the%20potential%20transmission%20period
Wyoming, Michigan 12/16/2021
1910.132(d)(1)(i)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.132#:~:text=1910.132(d)(1)(i,in%20the%20hazard%20assessment
1910.134(e)(1)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(e)(1,use%20a%20respirator
1910.502(f)(2)(i)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(f)(2)(i,accordance%20with%20%C2%A7%201910.134%20and
Oscode, Michigan 12/17/2021
1910.502(h)(1)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(h)(1,are%20in%20movement
Phoenix, Arizona 12/17/2021
1910.504(d)(3)(i)(B)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.504#:~:text=1910.504(d)(3)(i)(B,away%20from%20water%20or%20moisture
Bradford, Massachusetts 02/28/2022
1910.134(a)(2)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(a)(2,use%20a%20respirator
1910.134(f)(2)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(f)(2,least%20annually%20thereafter
1910.502(h)(1)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(h)(1,are%20in%20movement
1910.502(l)(3)(i)(A)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(l)(3)(i)(A,date(s)%20that%20contact%20occurred
1910.502(r)(1)(i)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(r)(1)(i,learning%20about%20the%20fatality
1910.502(r)(1)(ii)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(r)(1)(ii,the%20in%2Dpatient%20hospitalization
Baltimore, Maryland 03/01/2022
Baltimore, Maryland 03/07/2022
1904.29(b)(1)
https://www.osha.gov/laws-regs/regulations/standardnumber/1904/1904.29#:~:text=1904.29(b)(1,of%20the%20year
1904.29(b)(2)
https://www.osha.gov/laws-regs/regulations/standardnumber/1904/1904.29#:~:text=1904.29(b)(2,OSHA%20300%20Log
1904.29(b)(3)
https://www.osha.gov/laws-regs/regulations/standardnumber/1904/1904.29#:~:text=1904.29(b)(3,illness%20has%20occurred
1904.29(b)(7)(v)
https://www.osha.gov/laws-regs/regulations/standardnumber/1904/1904.29#:~:text=1904.29(b)(7)(v,1904.8%20for%20definitions)%3B%20and
1910.134(f)(2)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(f)(2,least%20annually%20thereafter
1910.134(k)(5)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(k)(5,following%20situations%20occur
1910.134(m)(2)(ii)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(m)(2)(ii,fit%20test%20is%20administered
1910.502(c)(5)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(c)(5,COVID%2D19%20plan
1910.502(f)(2)(i)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(f)(2)(ii,Note%20to%20paragraph
1910.502(l)(3)(i)(A)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(l)(3)(i)(A,date(s)%20that%20contact%20occurred
1910.502(l)(5)(iii)(A)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(l)(5)(iii)(A,l)(6)%20of%20this%20section
1910.502(n)(1)(ix)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(n)(1)(ix,g.%2C%20telework%2C%20flexible%20hours
1910.502(q)(2)(ii)(A)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.502#:~:text=1910.502(q)(2)(ii)(A,symptoms%2C%20if%20any%20were%20experienced
Cincinnati, Ohio 4/14/2022
1910.134(f)(2)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(f)(2,least%20annually%20thereafter
**Listed in PCD order**
1904.29(b)(1)
*What do I need to do to complete the OSHA 300 Log?* You must enter information about your business at the top of the OSHA 300 Log, enter a one or two line description for each recordable injury or illness, and summarize this information on the OSHA 300-A at the end of the year
1904.29(b)(2)
*What do I need to do to complete the OSHA 301 Incident Report?* You must complete an OSHA 301 Incident Report form, or an equivalent form, for each recordable injury or illness entered on the OSHA 300 Log.
1904.29(b)(3)
*How quickly must each injury or illness be recorded?* You must enter each recordable injury or illness on the OSHA 300 Log and 301 Incident Report within seven (7) calendar days of receiving information that a recordable injury or illness has occurred.
1904.29(b)(7)(v)
Needlestick injuries and cuts from sharp objects that are contaminated with another person’s blood or other potentially infectious material (see §1904.8 for definitions); and
1904.4(a)-(X3)
*Basic requirement*. Each employer required by this part to keep records of fatalities, injuries, and illnesses must record each fatality, injury and illness that
1904.7(b)(3)
***How do I record a work-related injury or illness that results in days away from work?*** When an injury or illness involves one or more days away from work, you must record the injury or illness on the OSHA 300 Log with a check mark in the space for cases involving days away and an entry of the number of calendar days away from work in the number of days column. If the employee is out for an extended period of time, you must enter an estimate of the days that the employee will be away, and update the day count when the actual number of days is known.
1910.132(d)(1)(i)
Select, and have each affected employee use, the types of PPE that will protect the affected employee from the hazards identified in the hazard assessment
1910.134(a)(2)
A respirator shall be provided to each employee when such equipment is necessary to protect the health of such employee. The employer shall provide the respirators which are applicable and suitable for the purpose intended. The employer shall be responsible for the establishment and maintenance of a respiratory protection program, which shall include the requirements outlined in paragraph (c) of this section. The program shall cover each employee required by this section to use a respirator.
1910.134(d)(1)(ii)
The employer shall select a NIOSH-certified respirator. The respirator shall be used in compliance with the conditions of its certification.
1910.134(e)(1)-(X2)
General. The employer shall provide a medical evaluation to determine the employee’s ability to use a respirator, before the employee is fit tested or required to use the respirator in the workplace. The employer may discontinue an employee’s medical evaluations when the employee is no longer required to use a respirator.
1910.134(e)(6)(i)
Obtain a written recommendation regarding the employee’s ability to use the respirator from the PLHCP. The recommendation shall provide only the following information:
1910.134(e)(6)(i)(A)
Any limitations on respirator use related to the medical condition of the employee, or relating to the workplace conditions in which the respirator will be used, including whether or not the employee is medically able to use the respirator.
1910.134(f)(2)-(X4)
The employer shall ensure that an employee using a tight-fitting facepiece respirator is fit tested prior to initial use of the respirator, whenever a different respirator facepiece (size, style, model or make) is used, and at least annually thereafter.
1910.134(g)(1)(ii)
If an employee wears corrective glasses or goggles or other personal protective equipment, the employer shall ensure that such equipment is worn in a manner that does not interfere with the seal of the facepiece to the face of the user.
1910.134(k)(5)
Retraining shall be administered annually, and when the following situations occur.
1910.134(m)(2)(ii)
The employer shall establish a record of the qualitative and quantitative fit tests administered to an employee including.
1910.502(c)(5)
The employer must seek the input and involvement of non-managerial employees and their representatives, if any, in the hazard assessment and the development and implementation of the COVID-19 plan.
1910.502(f)(2)(i)-(X2)
A respirator to each employee and ensure that it is provided and used in accordance with § 1910.134 and
1910.502(h)(1)-(X4)
The employer must ensure that each employee is separated from all other people by at least 6 feet when indoors unless the employer can demonstrate that such physical distancing is not feasible for a specific activity (*e.g.*, hands-on medical care). This provision does not apply to momentary exposure while people are in movement (*e.g.*, passing in hallways or aisles).
1910.502(j)(2)(i)
Clean high-touch surfaces and equipment at least once a day, following manufacturers’ instructions for application of cleaners; and
1910.502(l)(3)(i)(A)-(X3)
Notify each employee who was not wearing a respirator and any other required PPE and has been in close contact with that person in the workplace. The notification must state the fact that the employee was in close contact with someone with COVID-19 along with the date(s) that contact occurred.
1910.502(l)(5)(iii)(A)
The employer must continue to provide the benefits to which the employee is normally entitled and must also pay the employee the same regular pay the employee would have received had the employee not been absent from work, up to $1,400 per week, until the employee meets the return to work criteria specified in paragraph (l)(4)(iii) or (l)(6) of this section.
1910.502(n)(1)(ix)
Available sick leave policies, any COVID-19-related benefits to which the employee may be entitled under applicable federal, state, or local laws, and other supportive policies and practices (*e.g.*, telework, flexible hours);
1910.502(q)(2)(ii)(A)
The COVID-19 log must contain, for each instance, the employee’s name, one form of contact information, occupation, location where the employee worked, the date of the employee’s last day at the workplace, the date of the positive test for, or diagnosis of, COVID-19, and the date the employee first had one or more COVID-19 symptoms, if any were experienced.
1910.502(r)(1)(i)
Each work-related COVID-19 fatality within 8 hours of the employer learning about the fatality.
1910.502(r)(1)(ii)
When reporting COVID-19 fatalities and in-patient hospitalizations to OSHA in accordance with paragraph (r)(1) of this section, the employer must follow the requirements in 29 CFR 1904.39, except for 29 CFR 1904.39(a)(1) and (2) and (b)(6).
1910.504(d)(3)(i)(B)
The respirator has been stored in a breathable storage container (*e.g*., paper bag) for at least five calendar days between use and has been kept away from water or moisture;
1960.66(b)
Except as modified by this subpart, Federal agency injury and illness recording and reporting requirements shall comply with the requirements under 29 CFR Part 1904, subparts C, D, E, and G, except that the definition of “establishment” found in 29 CFR 1960.2(h) will remain applicable to Federal agencies.

“Although OSHA had not waived compliance with any of its requirements during the pandemic, the agency set forth temporary enforcement discretion policies that CSHOs could consider when enforcing OSHA standards, such as the Respiratory Protection standard, 29 CFR § 1910.134, and/or equivalent respiratory protection provisions of other health standards.”
https://www.osha.gov/laws-regs/standardinterpretations/2021-07-07#:~:text=Although%20OSHA%20had,other%20health%20standards.
LikeLike
The shocking thing about OSHA, Masks, and Respirators is that Respirators have usage restrictions based on Exposure Levels and their use around covid has not been based on those restrictions.
I can demonstrate with Benzene. OSHA feels that an employee can be exposed to 1 ppm without a respirator. If the level is above 1 ppm to 10 ppm, the employee must wear, at minimum, a Half Face Respirator with Organic Vapor Cartridges. Notice the 1 to 10 range. In order to use a Respirator, the environment can’t be Immediately Dangerous to Life and Health (IDLH). The IDLH for Benzene is 500 ppm.
But to determine how much Benzene is present, Testing of the Area needs done. Air Purifying Respirators are not permitted to be used where the atmosphere is IDLH (Except with the exception, perhaps, of Escape), where there is insufficient oxygen, and in areas that the Exposure Type AND Exposure Levels are not known.
There is an Assigned Protection Factor for Half Face Respirators of 10. They allow for the fact that up to 10% (or 1/10) of the Contaminant gets into the Facepiece (usually at the Face to Facepiece Seal) without being Filtered. That means that, ideally, wearing a Respirator for protection against Benzene, and allowing for the leakage that occurs, that only 1/10 of the Contaminant gets in past the Filter Media.
1/10 of 10 is 1. OSHA is essentially saying that even if the respirator leaks, and even if 1/10 of the contaminant gets in, that the level in the Facepiece would be 1 ppm, in other words, what you are permitted to be exposed to without a respirator.
If the level is 11 ppm, you can’t wear a Half Face, you need to use a Full Face Air Purifying Respirator. They have an Assigned Protection Factor of 50. 1/50th of the Contaminant may leak into the Facepiece, and that is 2%. For Benzene, you can be exposed to up to 50 ppm, and 2% of 50 ppm is, Drum Roll Please, 1 ppm.
Masks have no Face to Facepiece Seal, they can’t possibly be removing the contaminant. The original premise was that Masks stopped infectious droplets, but covid is assuredly Airborne, and that means that the Masks don’t Work and N95 Filtering Facepiece Respirators don’t work as well as we may think. Filtering Facepiece Respirators has an Assigned Protection Factor of 10. That means that they would allow up to 10% of the Contaminant into the Facepiece, and more if the Contaminant isn’t the proper size for the N95 Filtering Media, of 0.3 Microns or larger. covid is 0.125 Microns and Smaller, so more than 10% gets in. Best case, N95s remove 90%, and if they aren’t Fit Tested, If the wearer is not using the same Make, Model, and Size of Respirator they were Fit Tested for, has a beard, is not wearing it correctly, more than 10% may get in, how much covid is safe to breathe?
I wear an N95, I shave before needing to wear it. But I can’t see how Masks actually did anything substantially protective to the wearer. Well Known Respiratory Protection Science has been completely ignored to push a narrative.
LikeLiked by 1 person
On Sun, Aug 28, 2022, 6:48 PM Ma Tu wrote:
If only I knew a former 1 Star Army General who actually cared about the safety of our veterans via Veterans Affairs exposure.
To; my healthcare provider’s employer, my Mother and Father’s Dr.’s and Nurces, my kids and any other friends or loved ones I hold dear to my heart.
What is the #1 violation in healthcare? OSHA 29 CFR 1910.134(f)(2) look it up with information below. Download the checklist at https://info.kpa.io/hubfs/KPA%20Assets/EHS/KPA%20-%20EHS%20Checklist.pdf make sure you don’t have $$ thousands in fines for breaking OSHA COVID-19 Specific 5(a)1 citations. We are more than 2 years into a Hoax pandemic and Healthcare is breaking the laws your Employers and Political Leaders made laws to PREVENT, and was created NEVER TO BREAK. Sue the Political Leaders and get those idiots out of office and in PRISON where they belong.
Can you sue your boss for damages?
With SAFE TO WORK ACT. Yes you can as well as send him to prison for Gross Negligence by forcing employee’s to commit Wilful Neglect violations via policy and procedures that violate OSHA SAFETY LAWS. Those alternate plans also need OSHA approval via OSHA 1960.17
Can your Dr. use his lack of your medical condition as a discrimination tool?
Not without violating the Americans with Disabilities Act (ADA). Today they won’t even allow OSHA RESPITORY PROTECTION QUESTIONNAIRE in VETERANS AFFAIRS. That is to protect the individual from the side effects of negitive pressure masks and respiratory devices.
Check out Osha Factchecker Medical Terrorism infopage
Maybe it’s time to take the Dr. and politicians to court. Gross Negligence under TITLE 18 USC 1038.
NAICS Code: 62 Health Care and Social Assistance. Establishment Size: ALL sizes
https://www.osha.gov/pls/imis/citedstandard.naics?p_naics=62&p_esize=&p_state=FEFederal
Standard “Total”, citations 1,341 in healthcare during Inspections of 459 healthcare facilities with Penalty amounting to $3,879,662 for “All Standards cited for Health Care and Social Assistance”
Standard 19100134 “Respiratory Protection” number of citations found 707 of 1,341(52%) found during inspections 303 of 459 (66%) for a total Penalty amount of $2,183,424 of $3,879,662 (56%), in healthcare for “Respiratory Protection”.
Industry Profile for OSHA Standard 19100134 Establishment Size: All sizes
Standard: 19100134 Respiratory Protection.
https://www.osha.gov/pls/imis/industryprofile.stand?p_stand=19100134&p_state=FEFederal&p_type=2&p_esize=
Citations 2,190, Inspections 924, Penalty $4,442,986, Industry Classification “Total for All Industries”
Citations for respiratory protection. 707 of 2190 citations (all industries) at (32%) from inspections performed at 303 of 924 (all industries) at (32%) with total Penalty’s $2,183,424 (healthcare) of $4,442,986 (all industries) at (49%), Classification “Health Care and Social Assistance”
**The Employer Shall, means MANDATORY, failure to perform is Wilful Neglect. **
1910.134(a)(1)
In the control of those occupational diseases caused by breathing air contaminated with harmful dusts, fogs, fumes, mists, gases, smokes, sprays, or vapors, the primary objective shall be to prevent atmospheric contamination. This shall be accomplished as far as feasible by accepted engineering control measures (for example, enclosure or confinement of the operation, general and local ventilation, and substitution of less toxic materials). When effective engineering controls are not feasible, or while they are being instituted, appropriate respirators shall be used pursuant to this section.
1910.134(a)(2)
A respirator shall be provided to each employee when such equipment is necessary to protect the health of such employee. The employer shall provide the respirators which are applicable and suitable for the purpose intended. The employer shall be responsible for the establishment and maintenance of a respiratory protection program, which shall include the requirements outlined in paragraph (c) of this section. The program shall cover each employee required by this section to use a respirator.
1910.134(c)
Respiratory protection program. This paragraph requires the employer to develop and implement a written respiratory protection program with required worksite-specific procedures and elements for required respirator use. The program must be administered by a suitably trained program administrator. In addition, certain program elements may be required for voluntary use to prevent potential hazards associated with the use of the respirator. The Small Entity Compliance Guide contains criteria for the selection of a program administrator and a sample program that meets the requirements of this paragraph. Copies of the Small Entity Compliance Guide (below)
Click to access small-business.pdf
will be available on or about April 8, 1998 from the Occupational Safety and Health Administration’s Office of Publications, Room N 3101, 200 Constitution Avenue, NW, Washington, DC, 20210 (202-219-4667)
Industry Hygiene
Click to access training-library_industrial_hygiene.pdf
Most Frequently Cited
Click to access MFC_General_Industry_FY21.pdf
Covid-19 specific citations
https://www.osha.gov/enforcement/covid-19-data/inspections-covid-related-citations
Employees Rights
https://www.google.com/url?sa=t&source=web&rct=j&url=https://www.osha.gov/sites/default/files/publications/osha3021.pdf&ved=2ahUKEwjd-IHz3ej5AhU9EmIAHTqtDf0QFnoECBYQAQ&usg=AOvVaw0tTwCqbo0FZf_EfKcPDSaH
Inspection of respiratory protection plan
Click to access CPL_02-00-158.pdf
Field Operations Manual
Click to access CPL_02-00-150.pdf
Final Rules
https://www.osha.gov/laws-regs/federalregister/1998-01-08
“Bioaerosols” are airborne contaminants that are alive or were released from a living organism (OSHA Docket No. H-122; ACGIH Guidelines; Ex. 3-61C, page 1; 1994). Pulmonary effects associated with exposure to certain bioaerosols include rhinitis, asthma, allergies, hypersensitivity diseases, humidifier fever, and epidemics of infections including colds, viruses, tuberculosis, and Legionnaires Disease. Cardiovascular effects manifested as chest pain, and nervous system effects manifested as headache, blurred vision, and impaired judgment, have occurred in susceptible people following exposure to bioaerosols. Viral infections caused by the inhalation of bioaerosols can result in health effects that range in intensity from undetected or mild to more severe and even death. Bacterial infections resulting from inhalation of bacteria and their products cause a range of diseases, including tuberculosis, Legionnaires Disease, and hypersensitivity pneumonitis. Among workers in sewage treatment plants, health-related problems can be associated with occupational exposures to protozoa [Burge, H., 1990, “Bioaerosols: Prevalence and health effects in the indoor environment,” J. Allergy and Clinical Immunology; 86 (5); see also Exs. 3-61B and 3-61C in Docket No. H-122.] Allergic asthma and allergic rhinitis can be induced by chronic exposure to low levels of antigens. Hypersensitivity pneumonitis can occur when a worker inhales concentrated aerosols of particles released by bacteria, fungi, and protozoa (Exs. 3-61B and 3-61C in Docket No. H-122). In 1994, the Centers for Disease Control reported 41 deaths of workers for which there was evidence of work-related hypersensitivity pneumonitis (Work-Related Lung Disease Surveillance Report, 1994; USDHHS, CDC, DHHS (NIOSH) Number 94-120). Respirators to protect against the inhalation of biological agents are widely used in healthcare and other workplace settings where exposure to such agents presents a hazard to workers.
Respirators can also provide protection from oxygen-deficient atmospheres. Human beings must breathe oxygen in order to survive, and begin to suffer adverse health effects when the oxygen level of their breathing air drops below the normal atmospheric level. Below 19.5 percent oxygen by volume, air is considered oxygen-deficient. At concentrations of 16 to 19.5 percent, workers engaged in any form of exertion can rapidly become symptomatic as their tissues fail to obtain the oxygen necessary to function properly (Rom, W., Env. Occup. Med., 2nd ed; Little, Brown; Boston, 1992). Increased breathing rates, accelerated heartbeat, and impaired thinking or coordination occur more quickly in an oxygen-deficient environment. Even a momentary loss of coordination may be devastating to a worker if it occurs while the worker is performing a potentially dangerous activity, such as climbing a ladder. Concentrations of 12 to 16 percent oxygen cause tachypnea (increased breathing rates), tachycardia (accelerated heartbeat), and impaired attention, thinking, and coordination (e.g., Ex. 25-4), even in people who are resting.
At oxygen levels of 10 to 14 percent, faulty judgment, intermittent respiration, and exhaustion can be expected even with minimal exertion (Exs. 25-4 and 150).
Breathing air containing 6 to 10 percent oxygen results in nausea, vomiting, lethargic movements, and perhaps unconsciousness. Breathing air containing less than 6 percent oxygen produces convulsions, then apnea (cessation of breathing), followed by cardiac standstill. These symptoms occur immediately. Even if a worker survives the hypoxic insult, organs may show evidence of hypoxic damage, which may be irreversible (Exs. 25-4 and 150; also reported in: Rom, W., Environmental and Occupational Medicine, 2nd ed; Little, Brown; Boston, 1992).
A number of workplace conditions can lead to oxygen deficiency. Simple asphyxiants, or gases that are physiologically inert, can cause asphyxiation when present in high enough concentrations to lower the oxygen content in the air. Other toxic or chemical asphyxiants poison hemoglobin, cytochromes, or other enzyme systems (Rom, W., Environmental and Occupational Medicine, 2nd ed., Little, Brown, and Co., Boston, 1992). A number of asphyxiants are gases that can evolve from explosions, combustion, chemical reactions, or heating. A high-temperature electrical fire or arc welding accident causing a complete flashover in an enclosed area can temporarily eliminate oxygen from that area. Asphyxiation and the severe lung damage it can cause are major concerns for firefighters; of 30 firefighter deaths investigated by OSHA recently, five resulted from either asphyxiation, smoke inhalation, or flashovers (IMIS; 8 State plan states; 10/91-3/97). (See also mortality study of causes of death among firefighters, Guidotti, 37 JOEM 1348, 1995.)
In some cases, respirator use itself can cause illness and injury to employees. There are a number of physiological burdens that are associated with the use of certain types of respirators. The weight of the respirator, breathing resistances during both normal operation and if the air-purifying element is overloaded, and rebreathing exhaled air from respirator “dead space” can all increase the physiologic burden of respirator use (Exs. 113, 22-1, 64-427). Job and workplace conditions, such as the length of time a respirator must be worn, the level of physical exertion required of a respirator user, and environmental conditions, can also affect the physiological burden (Exs. 113, 64-363). In addition, workers who wear glasses or hearing aids may have problems achieving appropriate fit with some respirator facepieces.
Evidence of Adverse Health Effects From Respiratory Hazards. There is ample evidence that the previous standard was not doing an adequate job of protecting workers from these respiratory hazards, and that exposure to these hazards has continued to cause adverse health effects among exposed workers. An analysis of OSHA inspection data from 1976 through 1982, when the previous standard had been in effect for between five and eleven years (Ex. 33-5), found that in most cases (55.6 %) where respirators were used to protect employees from excessive levels of air contaminants, respiratory protection programs were deficient in one or more elements, thus increasing the potential for employee exposure. Even more significant was the fact that in 72.1 % of inspections in which an overexposure to a substance listed under 29 CFR 1910.1000 was cited, respirator use did not comply with the respiratory protection standard. OSHA performed a similar analysis of enforcement data for 1990-1996, and found similar levels of noncompliance. [See also Work-Related Lung Disease Surveillance Report, 1994; USDHHS, CDC, DHHS (NIOSH) Number 94-120.] The provisions of the new respirator standard are designed to regulate how an employer selects, maintains, fit tests, and trains employees in the proper use of respiratory equipment, and to provide employers with the tools needed to implement an effective respiratory protection program. OSHA has concluded that the new standard will eliminate many of the unnecessary illnesses and deaths described in this section.
Paragraph (e) — Medical Evaluations
The Committee recommended that a mandatory medical examination be required in accordance with ANSI Z88.2, and that the standard include a list of diseases and conditions that should be considered in determining an individual’s ability to wear a respirator. The final standard allows employers to rely on a screening questionnaire to identify employees with specified conditions that will require follow- up medical examinations. The questionnaire specifies medical conditions that OSHA has determined often relate to an employee’s ability to use a respirator. OSHA believes that this provision responds to the Committee’s concern.
Based on the comments of ACCSH and others, OSHA has decided to eliminate the proposed exemption for employees wearing respirators for no more than 5 hours per week, for the reasons explained below in the Summary and Explanation. The final rule also reflects the Committee’s recommendation that the medical opinion provided to the employer include only limitations on the employee’s ability to use a respirator.
The Committee recommended that OSHA add a provision to this paragraph requiring the employer to inform the person performing the medical examination of the atmospheric contaminants to which the employee would be exposed. The final standard meets this concern by requiring that the physician or other licensed health care professional (PLHCP) receive a copy of the employer’s written respirator program, and information about other environmental conditions an employee may encounter; this information will allow the medical professional to judge whether the employee is medically capable of wearing the respirator.
The final rule allows an employer who has, within the preceding 12 months, provided his or her employees with a medical evaluation that fulfills the requirements of the revised standard to rely on the results of that evaluation. OSHA believes that this provision is responsive to the Committee’s concern that limitations be placed on the “portability” of medical evaluations.
The Committee recommended that OSHA add a new provision to paragraph (e) to require that the employer provide a powered air- purifying respirator or atmosphere-supplying respirator to any employee found medically unable to wear a negative pressure respirator but otherwise able to perform the task to be done. The final standard requires the employer to provide a PAPR to an employee when the PLHCP informs the employer that the employee has a medical condition that may place the employee’s health at increased risk of material impairment if the employee uses a negative pressure respirator (paragraph (e)(6)(ii)) and is thus responsive to the Committee’s concern.
Extras
http://niosh.dnacih.com/nioshdbs/respprot/www.osha-slc.gov/SLTC/respiratory_advisor/oshafiles/respiratory2.html
Covid 19 specific cited violations in healthcare.
https://www.osha.gov/enforcement/covid-19-data/inspections-covid-related-citations
1910.134(f)(2)
https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134#:~:text=1910.134(f)(2,least%20annually%20thereafter
1910.134(c)(1)
In any workplace where respirators are necessary to protect the health of the employee or whenever respirators are required by the employer, the employer shall establish and implement a written respiratory protection program with worksite-specific procedures. The program shall be updated as necessary to reflect those changes in workplace conditions that affect respirator use. The employer shall include in the program the following provisions of this section, as applicable:
1910.134(c)(1)(i)
Procedures for selecting respirators for use in the workplace;
1910.134(c)(1)(ii)
Medical evaluations of employees required to use respirators;
1910.134(c)(1)(iii)
Fit testing procedures for tight-fitting respirators;
1910.134(c)(1)(iv)
Procedures for proper use of respirators in routine and reasonably foreseeable emergency situations;
1910.134(c)(1)(v)
Procedures and schedules for cleaning, disinfecting, storing, inspecting, repairing, discarding, and otherwise maintaining respirators;
1910.134(c)(1)(vi)
Procedures to ensure adequate air quality, quantity, and flow of breathing air for atmosphere-supplying respirators;
1910.134(c)(1)(vii)
Training of employees in the respiratory hazards to which they are potentially exposed during routine and emergency situations;
1910.134(c)(1)(viii)
Training of employees in the proper use of respirators, including putting on and removing them, any limitations on their use, and their maintenance; and
1910.134(c)(1)(ix)
Procedures for regularly evaluating the effectiveness of the program.
1910.134(c)(2)
Where respirator use is not required:
1910.134(c)(2)(i)
An employer may provide respirators at the request of employees or permit employees to use their own respirators, if the employer determines that such respirator use will not in itself create a hazard. If the employer determines that any voluntary respirator use is permissible, the employer shall provide the respirator users with the information contained in appendix D to this section (“Information for Employees Using Respirators When Not Required Under the Standard”); and
1910.134(c)(2)(ii)
In addition, the employer must establish and implement those elements of a written respiratory protection program necessary to ensure that any employee using a respirator voluntarily is medically able to use that respirator, and that the respirator is cleaned, stored, and maintained so that its use does not present a health hazard to the user. Exception: Employers are not required to include in a written respiratory protection program those employees whose only use of respirators involves the voluntary use of filtering facepieces (dust masks).
1910.134(c)(3)
The employer shall designate a program administrator who is qualified by appropriate training or experience that is commensurate with the complexity of the program to administer or oversee the respiratory protection program and conduct the required evaluations of program effectiveness.
1910.134(c)(4)
The employer shall provide respirators, training, and medical evaluations at no cost to the employee.
1960.1(e)
Executive Order 12196 and these basic program elements apply to all agencies of the Executive Branch. They apply to all Federal employees. They apply to all working conditions of Federal employees except those involving uniquely military equipment, systems, and operations.
An agency head may apply an alternate standard where deemed necessary, and shall, after consultation with employees or their representatives, including appropriate occupational safety and health committees, notify the Secretary and request approval of such alternate standards.
1960.17(a)
Any request by the head of the agency for an alternate standard shall be transmitted to the Secretary.
1960.17(b)
Any such request for an alternate standard shall not be approved by the Secretary unless it provides equivalent or greater protection for affected employees. Any such request shall include:
1960.17(b)(1)
A statement of why the agency cannot comply with the OSHA standard or wants to adopt an alternate standard;
1960.17(b)(2)
A description of the alternate standard;
1960.17(b)(3)
An explanation of how the alternate standard provides equivalent or greater protection for the affected employees;
1960.17(b)(4)
A description of interim protective measures afforded employees until a decision is rendered by the Secretary of Labor; and
1960.17(b)(5)
A summary of written comments, if any, from interested employees, employee representatives, and occupational safety and health committees.
1960.28(c)
Any employee or representative of employees, who believes that an unsafe or unhealthful working condition exists in any workplace where such employee is employed, shall have the right and is encouraged to make a report of the unsafe or unhealthful working condition to an appropriate agency safety and health official and request an inspection of such workplace for this purpose. The report shall be reduced to writing either by the individual submitting the report or, in the case of an oral notification, by the above official or other person designated to receive the reports in the workplace. Any such report shall set forth the grounds for the report and shall contain the name of the employee or representative of employees. Upon the request of the individual making such report, no person shall disclose the name of the individual making the report or the names of individual employees referred to in the report, to anyone other than authorized representatives of the Secretary. In the case of imminent danger situations, employees shall make reports by the most expeditious means available.
1960.28(d)(1)
Each report of an existing or potential unsafe or unhealthful working condition should be recorded on a log maintained at the establishment. If an agency finds it inappropriate to maintain a log of written reports at the establishment level, it may avail itself of procedures set forth in §1960.71. A copy of each report received shall be sent to the appropriate establishment safety and health committee.
1960.28(d)(2)
A sequentially numbered case file, coded for identification, should be assigned for purposes of maintaining an accurate record of the report and the response thereto. As a minimum, each establishment’s log should contain the following information: date, time, code/reference/file number, location of condition, brief description of the condition, classification (imminent danger, serious or other), and date and nature of action taken.
1960.28(d)(3)
Executive Order 12196 requires that agency inspections be conducted within 24 hours for employee reports of imminent danger conditions, within three working days for potentially serious conditions, and within 20 working days for other than serious safety and health conditions. However, an inspection may not be necessary if, through normal management action and with prompt notification to employees and safety and health committees, the hazardous condition(s) identified can be abated immediately.
1960.31(a)
The Secretary or the Secretary’s representatives are authorized to conduct, when the Secretary deems necessary, announced or unannounced inspections in the following situations:
1960.31(a)(1)
Where an agency has not established occupational safety and health committees or where committees no longer operate in conformance to the requirements of subpart F of this part;
1960.46(a)
The head of each agency shall establish procedures to assure that no employee is subject to restraint, interference, coercion, discrimination or reprisal for filing a report of an unsafe or unhealthful working condition, or other participation in agency occupational safety and health program activities, or because of the exercise by such employee on behalf of himself or herself or others of any right afforded by section 19 of the Act, Executive Order 12196, or this part. These rights include, among other, the right of an employee to decline to perform his or her assigned task because of a reasonable belief that, under the circumstances the task poses an imminent risk of death or serious bodily harm coupled with a reasonable belief that there is insufficient time to seek effective redress through normal hazard reporting and abatement procedures established in accordance with this part.
1960.46(b)
Based on the Secretary’s evaluation of agencies’ procedures for protecting employees from reprisal, the Secretary shall report to the President by September 30, 1982 his findings and recommendations for improvements in procedures for the investigation and resolution of allegations of reprisal.
1960.71(b)
The Secretary will submit to the President by January 1 of each year a summary report of the status of the occupational safety and health of Federal employees based on agency reports, evaluations of individual agency progress and problems in correcting unsafe or unhealthful working conditions, and recommendations for improving their performance.
1960.79
Agency heads shall develop and implement a program of self-evaluations to determine the effectiveness of their occupational safety and health programs. The self-evaluations are to include qualitative assessments of the extent to which their agency safety and health programs are:
1960.79(a)
Developed in accordance with the requirements set forth in Executive Order 12196 and this part and,
1960.79(b)
Implemented effectively in all agency field activities.
The final standard on respiratory protection does not concern “Environmental health risks and safety risks” to children as defined under the Executive order. The respirator standard is only concerned with means of limiting employee exposures to toxic substances. The Agency believes, therefore, that the requirement noted above to provide OIRA with certain information does not apply since the respiratory protection standard is not a “covered regulatory action” under Executive Order 13045.
Section 6(b) (8) of the OSH Act requires OSHA to explain “why a rule promulgated by the Secretary differs substantially from an existing national consensus standard,” by publishing “a statement of the reasons why the rule as adopted will better effectuate the purposes of the Act than the national consensus standard.” In compliance with the requirement, the Agency has reviewed the standards proposed through this rulemaking with reference to the ANSI Z88.2-1992 standard for Respiratory Protection. OSHA has discussed the relationship between individual regulatory provisions and the corresponding consensus standards in the Summary and Explanation of the final rule.
II. Pertinent Legal Authority
The purpose of the Occupational Safety and Health Act, 29 U.S.C. 651 et seq. (“the Act”) is to “assure so far as possible every working man and woman in the nation safe and healthful working conditions and to preserve our human resources.” 29 U.S.C. 651(b). To achieve this goal, Congress authorized the Secretary of Labor to promulgate and enforce occupational safety and health standards. U.S.C. 655(a) (authorizing summary adoption of existing consensus and Federal standards within two years of Act’s enactment), 655(b) (authorizing promulgation of standards pursuant to notice and comment), 654(b) (requiring employers to comply with OSHA standards).
All standards must be highly protective. See 58 FR 16614-16615; LOTO III, 37 F.3d at 668. However, standards regulating exposure to toxic substances or hazardous physical agents must also meet the “feasibility mandate” of Section 6(b)(5) of the Act, 29 U.S.C. 655(b)(5). Section 6(b)(5) requires OSHA to select “the most protective standard consistent with feasibility” that is needed to reduce significant risk when regulating these hazards. ATMI, 452 U.S. at 509.
References
Senator Bill Frist video https://www.c-span.org/video/?190239-1/pandemic-flu-preparedness
August 10, 1989
https://www.osha.gov/laws-regs/standardinterpretations/1989-08-10
Approval of alternate standards pursuant to OSHA regulation. Veterans Administration:
Request for approval—March 7, 1985.
March 9, 1995
https://www.osha.gov/laws-regs/standardinterpretations/1995-03-09
October 5, 1998
https://www.osha.gov/laws-regs/standardinterpretations/1998-10-05
December 2, 1998
https://www.osha.gov/laws-regs/standardinterpretations/1998-12-02
December 23, 1998
https://www.osha.gov/laws-regs/standardinterpretations/1998-12-23
January 4, 1999
https://www.osha.gov/laws-regs/standardinterpretations/1999-01-04-1
January 29, 1999
https://www.osha.gov/laws-regs/standardinterpretations/1999-01-29
NIOSH approval for this situation is not, as you suggest, purely academic. There is the potential that the use of these two respirators together could affect the protection factors of each other due to their mutual interference. This interference may not always be obvious. As we stated in the first letter, the only way to determine this for sure would be to submit all respirator components for approval as required by NIOSH. For this reason, we continue to view dual use of respirators as a potential hazard.
August 27, 1999
https://www.osha.gov/laws-regs/standardinterpretations/1999-08-27
October 1, 1999
https://www.osha.gov/laws-regs/standardinterpretations/1999-10-01
June 12, 2002
https://www.osha.gov/laws-regs/standardinterpretations/2002-06-12-0
March 7, 2003
https://www.osha.gov/laws-regs/standardinterpretations/2003-03-07-0
February 5, 2004
https://www.osha.gov/laws-regs/standardinterpretations/2004-02-05
Fit testing requirements for employees who wear respirators to protect against M. Tuberculosis, SARS, Smallpox, and Monkeypox.
February 6, 2006
https://www.osha.gov/laws-regs/standardinterpretations/2006-02-06-0
April 10, 2007
https://www.osha.gov/laws-regs/standardinterpretations/2007-04-04
The Respiratory Protection standard, 29 CFR 1910.134, requires employers to ensure their employees perform a user seal check each time they don a tight-fitting respirator using either the “user seal check” procedures in Appendix B-1 or equally effective procedures recommended by the respirator manufacturer.
June 2, 2009
https://www.osha.gov/laws-regs/standardinterpretations/2009-06-02-0
July 14, 2009
https://www.osha.gov/laws-regs/standardinterpretations/2009-07-14-0
November 22, 2011
https://www.osha.gov/laws-regs/standardinterpretations/2011-11-22-0
Question 7: If OSHA considers the N95 filtering facepiece a respirator covered by the respiratory protection standard, what parts of paragraph (h) involving “maintenance and care of respirators” are applicable? Does the employer have to comply with Appendix B-2 involving “Respirator Cleaning Procedures”?
Response: The N95 filtering facepiece respirator is a “disposable respirator.” It must be discarded after use, or when it becomes damaged or soiled. It cannot be cleaned and disinfected according to the method described in Appendix B-2. OSHA is presently not aware of any alternate procedures provided by respirator manufacturers in their user instructions that would allow for cleaning and disinfecting their filtering facepiece respirators.
September 14, 2012
https://www.osha.gov/laws-regs/standardinterpretations/2012-09-14
February 8, 2016
https://www.osha.gov/laws-regs/standardinterpretations/2016-02-08
December 20, 2017 https://www.osha.gov/laws-regs/standardinterpretations/2017-12-20
April 25, 2018
https://www.osha.gov/laws-regs/standardinterpretations/2018-04-24
Feb 4, 2020 FDA EUA’s first came out. Cannot find link
March 14, 2020 https://www.osha.gov/laws-regs/standardinterpretations/2020-03-14
April 3, 2020 https://www.osha.gov/laws-regs/standardinterpretations/2020-04-03
April 8, 2020
https://www.osha.gov/laws-regs/standardinterpretations/2020-04-08
April 16, 2020
https://www.osha.gov/laws-regs/standardinterpretations/2020-04-16
May 19, 2020
https://www.osha.gov/memos/2020-05-19/updated-interim-enforcement-response-plan-coronavirus-disease-2019-covid-19
May 27, 2021
https://www.fda.gov/medical-devices/letters-health-care-providers/update-fda-recommends-transition-use-non-niosh-approved-and-decontaminated-disposable-respirators
Update: FDA Recommends Transition from Use of Non-NIOSH-Approved and Decontaminated Disposable Respirators – Letter to Health Care Personnel and Facilities
For Immediate Release:
June 30, 2021 FDA In Brief: FDA Revokes Emergency Use Authorizations for Certain Respirators and Decontamination Systems as Access to N95s Increases Nationwide.
https://www.fda.gov/news-events/press-announcements/fda-brief-fda-revokes-emergency-use-authorizations-certain-respirators-and-decontamination-systems
July 7, 2021
https://www.osha.gov/laws-regs/standardinterpretations/2021-07-07
July 12, 2021
https://www.fda.gov/media/135763/download
Respirators on the NIOSH Certified Equipment List are authorized under the Emergency Use Authorization (EUA) for NIOSH-Approved Air Purifying Respirators for Use in Health Care Settings During Response to the COVID-19 Public Health Emergency.
August 25, 2021
https://www.fda.gov/medical-devices/medical-device-recalls/stop-using-certain-n95-respirators-manufactured-shanghai-dasheng-letter-health-care-providers
Stop Using Certain N95 Respirators Manufactured by Shanghai Dasheng – Letter to Health Care Providers
December 16, 2021
https://www.osha.gov/laws-regs/standardinterpretations/2021-12-16
Respiratory protection against COVID-19 for employees with religiously mandated facial hair
December 27, 2021
https://www.osha.gov/coronavirus/ets/
August 26, 2022
https://www.fda.gov/medical-devices/letters-health-care-providers/update-fda-no-longer-authorizes-use-non-niosh-approved-or-decontaminated-disposable-respirators
Update: FDA No Longer Authorizes Use of Non-NIOSH-Approved or Decontaminated Disposable Respirators – Letter to Health Care Personnel and Facilities
CDC is full of bad information
https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/about-face-coverings.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fyour-health%2Feffective-masks.html
On page 43 of 134
https://www.google.com/url?sa=t&source=web&rct=j&url=https://www.api.org/-/media/Files/Certification/ICP/ICP-Certification-Programs/1169_2017_GovRefDocs/1169_USA_29-CFR-1910_OSHA_Eff-04-2017.pdf%3Fla%3Den%26hash%3D2CAFB8F272F0263111115A7F302849701F406DA3&ved=2ahUKEwjcuMuBlOr5AhWpkYkEHalGAz04FBAWegQIDRAB&usg=AOvVaw2ii1xaBx2RG3MclKYAGinB
(ii) In addition, the employer must establish and implement those elements of a written respiratory protection program necessary to ensure that any employee using a respirator voluntarily is medically able to use that respirator, and that the respirator is cleaned, stored, and maintained so that its use does not present a health hazard to the user. Exception: Employers are not required to include in a written respiratory protection program those employees whose only use of respirators involves the voluntary use
of filtering facepieces (dust masks).
(3) The employer shall designate a program administrator who is qualified by appropriate training or experience that is commensurate with the complexity of the program to administer or oversee the
respiratory protection program and conduct the required evaluations of program effectiveness.
(4) The employer shall provide respirators, training, and medical evaluations at no cost to the employee.
(d) Selection of respirators. This paragraph requires the employer to evaluate respiratory hazard(s) in the workplace, identify relevant workplace and user factors, and base respirator selection on these factors. The paragraph also specifies appropriately protective respirators for use in IDLH atmospheres, and limits the selection and use of air-purifying respirators.
(1) General requirements.
(i) The employer shall select and provide an appropriate respirator based on the respiratory hazard(s) to which the worker is exposed and workplace and user factors that affect respirator performance and reliability.
(ii) The employer shall select a NIOSH-certified respirator. The respirator shall be used in compliance with the conditions of its certification.
Pages 39-85 are all about OSHA Respitory Protection and 79 to 84 is your Respitory Protection Medical Questionnaire used in conjunction with a Medical Evaluation to determine your level of safety.
Missing from OSHA databanks
http://intranet.osha.gov/compliance/sig_pdf/sigcaseprocedures2004.html
In 2020 Letters to Health Care Providers
https://www.fda.gov/medical-devices/letters-health-care-providers/2020-letters-health-care-providers
This page is not found
Surgical Mask and Gown Conservation Strategies – Letter to Healthcare Providers.
V/r
Matthew Aaron Tuinstra
Ex-military Emergency Medical Assistance Team, HACCP Manager, Culinary Specialists, Submarine Fire Fighter and Damage Control, Biological Evaluation and Hazard Assessments Analysis Specialists.
oshafactchecker@gmail.com
Ixoyc.zwntwn@gmail.com
(860)800-6679 or (860)451-9588
LikeLike