Perfect practice makes perfect, poor practicing makes fools
Author Archives: Matthew A. T.
Senator Bill Frist
https://www.c-span.org/video/?190239-1/pandemic-flu-preparedness
December 20, 2017
https://www.osha.gov/laws-regs/standardinterpretations/2017-12-20
March 14, 2020
https://www.osha.gov/laws-regs/standardinterpretations/2020-03-14
April 3, 2020
https://www.osha.gov/laws-regs/standardinterpretations/2020-04-03
End the pandemic hoax by OSHA FactChecker
https://oshafactchecker.law.blog/
https://youtu.be/9t74xtVNoDw
is your boss in compliance? or was he fooled into being non-compliant?
here is sine communication I’ve had with OSHA about a friend who was forced to use N95’s without training fut testing, and medical evaluations. I would call ot criminal Gross Negligence.
On Fri, Jan 20, 2023, 3:13 PM Ma Tu
<oshafactchecker@gmail.com>
wrote: The letter in the mail came today..from Brown, Derek J. Sent Dec 22, 2022
Which states employees at the Norwich vet center are not required to use respirators, which is false. I have spoken to several employees who state that Jamie Harnandez the Director first forced them to use loosfitting surgical masks, which isn’t allowed because of
OSHA 29 CFR 1910.134(f)(2) The employer shall ensure that an employee using a tight-fitting facepiece respirator is fit tested prior to initial use of the respirator, whenever a different respirator facepiece (size, style, model or make) is used, and at least annually thereafter.
So the CDC & FDA wants people to break the law while OSHA collects $8 million from Employers who allow it to happen? which is cited as the #1 citation for COVID-19 Specific citations during the pandemic and the Respiratory Protection program went from an average 4th/5th on top 10 most violated (and is a yearly report to the POTUS.
If the Employer/Director (Jamie Harnandez) allows them to use those Loose fitting masks he shall make sure it doesn’t become a hazard to the employee using it or other employees, via
OSHA 29 CFR Appendix (D-1) which is under OSHA 29 CFR 1910.134(c)(2)(i) An employer may provide respirators at the request of employees or permit employees to use their own respirators, if the employer determines that such respirator use will not in itself create a hazard. If the employer determines that any voluntary respirator use is permissible, the employer shall provide the respirator users with the information contained in appendix D to this section (“Information for Employees Using Respirators When Not Required Under the Standard”); and Found Here
Which states within it’s standard and Interpretations from OSHA that. Which states “However, surgical masks may not be used in lieu of required respiratory protection. Surgical masks are not considered respirators by OSHA and, as such, are not covered by 29 CFR 1910.134. They are fluid resistant, disposable, and loose-fitting protection that create a physical barrier between the mouth and nose of the wearer and potential contaminants in the immediate environment.”
However, surgical masks do not seal tightly to the wearer’s face, nor do they provide a reliable level of protection from inhaling smaller airborne particles.
FROM: PATRICK J. KAPUST, Acting DirectorDirectorate of Enforcement Programs
THROUGH: AMANDA EDENSDeputy Assistant Secretary
MEMORANDUM FOR: REGIONAL ADMINISTRATORSSTATE PLAN DESIGNEES,
Which states “This memorandum also includes policy changes regarding enforcement discretion for periodic respiratory protection equipment shortages and associated constraints (i.e., fit-testing supplies and provision of related services) during the COVID-19 pandemic. Although OSHA had not waived compliance with any of its requirements during the pandemic, the agency set forth temporary enforcement discretion policies that CSHOs could consider when enforcing OSHA standards, such as the Respiratory Protection standard, 29 CFR § 1910.134, and/or equivalent respiratory protection provisions of other health standards”
At some point those employees stated that N95 were issued to them without Training, without Fit Testing and without Medical Evaluations, which alone for each employee is a safery violation and more than $14,000 a citation and considered Wilful Neglest under OSHA’s standards. Today those 3 violations is upwards of $42,000 per employee.
If the VA employees in medical setting are required to wear a disposable protective medical mask per VA regulations, where is the OSHA 29 CFR 1960.17 Alternate standard request send to OSHA allowing and approving it prior to implementation.
Why is the standard OSHA 29 CFR 1960.46(a) being violated where VA is firing people who, for health reasons, refuse to wear a mask and or FFR Respitory when they haven’t performed the proper Medical Evaluations with the questionnaire OSHA 29 CFR 1910.134 Appendix(c)
which lists the many medical conditions that are designed to protect the Employee from those Employers like
Part A. Section 2. (Mandatory) Questions 1 through 9 below must be answered by every employee who has been selected to use any type of respirator (please circle “yes” or “no”).
1. Do you currently smoke tobacco, or have you smoked tobacco in the last month: Yes/No
2. Have you ever had any of the following conditions?a. Seizures: Yes/Nob. Diabetes (sugar disease): Yes/Noc. Allergic reactions that interfere with your breathing: Yes/Nod. Claustrophobia (fear of closed-in places): Yes/Noe. Trouble smelling odors: Yes/No
3. Have you ever had any of the following pulmonary or lung problems?
a. Asbestosis: Yes/No
b. Asthma: Yes/No
c. Chronic bronchitis: Yes/No
d. Emphysema: Yes/No
e. Pneumonia: Yes/No
f. Tuberculosis: Yes/No
g. Silicosis: Yes/Noh. Pneumothorax (collapsed lung): Yes/No
i. Lung cancer: Yes/No
j. Broken ribs: Yes/No
k. Any chest injuries or surgeries: Yes/Nol. Any other lung problem that you’ve been told about: Yes/No
4. Do you currently have any of the following symptoms of pulmonary or lung illness?
a. Shortness of breath: Yes/Nob. Shortness of breath when walking fast on level ground or walking up a slight hill or incline: Yes/No
c. Shortness of breath when walking with other people at an ordinary pace on level ground: Yes/No
d. Have to stop for breath when walking at your own pace on level ground: Yes/No
e. Shortness of breath when washing or dressing yourself: Yes/No
f. Shortness of breath that interferes with your job: Yes/No
g. Coughing that produces phlegm (thick sputum): Yes/No
h. Coughing that wakes you early in the morning: Yes/No
i. Coughing that occurs mostly when you are lying down: Yes/No
j. Coughing up blood in the last month: Yes/No
k. Wheezing: Yes/No
l. Wheezing that interferes with your job: Yes/No
m. Chest pain when you breathe deeply: Yes/No
n. Any other symptoms that you think may be related to lung problems: Yes/No
5. Have you ever had any of the following cardiovascular or heart problems?
a. Heart attack: Yes/No
b. Stroke: Yes/No
c. Angina: Yes/No
d. Heart failure: Yes/No
e. Swelling in your legs or feet (not caused by walking): Yes/No
f. Heart arrhythmia (heart beating irregularly): Yes/No
g. High blood pressure: Yes/No
h. Any other heart problem that you’ve been told about: Yes/No
6. Have you ever had any of the following cardiovascular or heart symptoms?
a. Frequent pain or tightness in your chest: Yes/No
b. Pain or tightness in your chest during physical activity: Yes/No
c. Pain or tightness in your chest that interferes with your job: Yes/No
d. In the past two years, have you noticed your heart skipping or missing a beat: Yes/No
e. Heartburn or indigestion that is not related to eating: Yes/No
f. Any other symptoms that you think may be related to heart or circulation problems: Yes/No
7. Do you currently take medication for any of the following problems?
a. Breathing or lung problems: Yes/No
b. Heart trouble: Yes/No
c. Blood pressure: Yes/No
d. Seizures: Yes/No
8. If you’ve used a respirator, have you ever had any of the following problems? (If you’ve never used a respirator, check the following space and go to question 9:)
a. Eye irritation: Yes/No
b. Skin allergies or rashes: Yes/No
c. Anxiety: Yes/No
d. General weakness or fatigue: Yes/No
e. Any other problem that interferes with your use of a respirator: Yes/No
9. Would you like to talk to the health care professional who will review this questionnaire about your answers to this questionnaire: Yes/No
I have tried to file an SEC Whistleblower case aginst the VA in Dec of 2021 & March of 2022, where the VA Whistleblower Analysts, Sam Glover, from PA said they were flowing FDA guidlines for EUA’s that have already been revoked (July 6th, 2021), and where FDA standards do not overrule OSHA and the Final Rule of 1998 by Suprime Court which state ample amounts of information for these rules and regulations.
This complain is correct, and their use is not in compliance with OSHA, all attempts to correct the situation have been blocked which is TITLE 18 USC 2071 violation which is up to 5 years in Prison.
As far as purchasing them masks over the counter at CVS, those EUS’s Sent out in Feb 4th of 2020 stated they still needed to be equivalent to NIOSH, if it wasnt equivalent to the NIOSH standard it broke FDA MOU’s for aporving masks (class II medical devices) which still had to have testing vs bacterial filtration efficiency (which no loose fit mask has ever passed the NIOSH certification), even NIOSH Regulations have been made to never test them again.
Surgical Masks also must be thrown away after each; use, task, or each patient, not walk room to room. Those EUA’s from the FDA allowing the sale of masks in stores has also been revoked because we now have plunty supple of peoper N95 respiratory protection available in the Huky 7th, 2021 memorandum aent to Administrators and state plan dessignees.
I have also been discriminated aginst by Jamie Harnandez under the ADA about the issue and my services even over the Phone have been blocked, when I have been asking for help with the Councelers, as my last counselor has just retired.
I have also filed a grevance about the VA when Dr. Kauffman threatened me for talking about the masks when he told me he puts it in his pocket when not walking the halls, which was 100% aginst all the spandards given by OSHA, CDC, & FDA altogether. The letter from from Brown, Derek J. Also says “The VA has medical has policies in place for medical accommodations” this doesn’t remove the requirement to have it on file, and the training records, the Fit Yesting, or the Medical Evaluations like a letter from the PLHCP which will state the use and limitations for the individual.
Those are based on his medical health, and if he fails he cannot wear ANY MASK, because it can be a danger to his health if having and medical conditions listed in OSHA 29 CFR 1910.134 Appendix (c) while the PLHCP is supposed to use American National Standard Index (ANSI) Z88.2-Z88.6 Respiratory Protection standard and Evaluations.
This is Gross Criminal Negligence under the SAFE TO WORK ACT and those standards were designed to keep employees from being unsanitary and unsafe.
I have the training to be a Respiratory Protection Administrator and have been a HACCP Administrator, Compliance Officer, Instructor for Sanitation and Cross-contamination Prevention, Emergency Medical Assistance Team, Certified Professional Food Manager, Fire Fighter (and much more) while working on Submarines in the Navy.
V/r Matthew A. Tuinstra
I would like to know why OSHA neglected to take the issues adress and do a proper Investigation using the Field Operations Manual as I had to use on Submarines on a regular basis?
Are my CHSO’s guilty of Gross Criminal Negligence? Cause this doesn’t look good for any individual person to have this on his record. Remember TITLE 18 USC 1038 Fasle, Hoax, and Misleading information is a 5-20 year prison sentence and even Dr. Fauci and Dr. Robert Redfield can easily be exposed for the crimes.
Please adress those items one by one and let me know why you do not do an Inspection, because this is a form of Medical Terrorism from the Employer/Director of Norwich Veterans Center as it is his responsibility to follow those laws not make policy that was never approved under OSHA 29 CFR 1960.17 and is non-compliance ans not at all congruent with OSHA.
I have made many binders of all this information and copied most of those Documents for my personal Respiratory Protection program binders many times, and building another for personal use.
God Bless,Matthew Aaron Tuinstra.
no responce as of January 28, 2023 so I send them another email.
Did I scare you away? I have Rights to seek Redress for this issue. Under the 1st Amendment, you know the right to free speech, freedom of religon and to petition the Government for a redress of grievances.
Under the 9th Ammendment, no matter how many rights given to society, nobody can deny or disparage. Just so you know disparage means: cannot make it seem worthless.
Under OSHA 29 CFR 1910.134(f)(2) The employer shall ensure that an employee using a tight-fitting facepiece respirator is fit tested prior to initial use of the respirator, whenever a different respirator facepiece (size, style, model or make) is used, and at least annually thereafter.
Which is also the #1 cited COVID-19 Specific violation, and theirs almost 3 years of them citine it af $14,000+ for each occurrence.
Theirfor if Veterans Affairs has a Policy for Employees to break this right and Protection under section 19 of the OSHA Act.
Anyone who tells me a loose fit mask is biological protection is liable under TITLE 18 USC 1038, which is False, Hoax, and Misleading information about Biological hazards, because they do not know my underlying medical issues.
I have Rights and protections that “No Employer, No employee, No Goverment agency can abuse”, not even the sitting POTUS has the authority to force me, or anyone else for that matter, just use
OSHA 29 CFR 1960.46(a) The head of each agency shall establish procedures to assure that no employee is subject to restraint, interference, coercion, discrimination or reprisal for filing a report of an unsafe or unhealthful working condition, or other participation in agency occupational safety and health program activities, or because of the exercise by such employee on behalf of himself or herself or others of any right afforded by section 19 of the Act, Executive Order 12196, or this part. These rights include, among other, the right of an employee to decline to perform his or her assigned task because of a reasonable belief that, under the circumstances the task poses an imminent risk of death or serious bodily harm coupled with a reasonable belief that there is insufficient time to seek effective redress through normal hazard reporting and abatement procedures established in accordance with this part.
I have also spoken to Employees who have been forced to wear a mask, first 2 years it was loose fit (which has been cited by CHSO’s all pandemic long in healthcare) then it was switched to N95’s, without; fitchecks, training, and medical evaluations. 1910.134(f)Fit testing. This paragraph requires that, before an employee may be required to use any respirator with a negative or positive pressure tight-fitting facepiece, the employee must be fit tested with the same make, model, style, and size of respirator that will be used. This paragraph specifies the kinds of fit tests allowed, the procedures for conducting them, and how the results of the fit tests must be used.
1910.134(f)(3)The employer shall conduct an additional fit test whenever the employee reports, or the employer, PLHCP, supervisor, or program administrator makes visual observations of, changes in the employee’s physical condition that could affect respirator fit. Such conditions include, but are not limited to, facial scarring, dental changes, cosmetic surgery, or an obvious change in body
weight1910.134(e)(1) General. The employer shall provide a medical evaluation to determine the employee’s ability to use a respirator, before the employee is fit tested or required to use the respirator in the workplace. The employer may discontinue an employee’s medical evaluations when the employee is no longer required to use a respirator.
1910.134(c)(1)(ii) Medical evaluations of employees required to use respirators.
I am also well aware of unlawful modifications to OSHA Standards and interpretations, specifically in regards to
Which removed very little information but the info removed was “NOTE: however Healthcare personnel shall not use facemasks as biological protection FFR’s” which now states “However, surgical masks do not seal tightly to the wearer’s face, nor do they provide a reliable level of protection from inhaling smaller airborne particles”. Not much of a change but a change it was a change indeed and a violation of TITLE 18 USC 2071 (Concealment, removal, or mutilation generally)
My friend who is employed, told me workers are being fired for non-compliance to those bad police which not only violated
OSHA 29 CFR 1960.46(a)[ listed above] but also the alternate policy must be equal or more protective than OSHA, then sent to OSHA under 1960.17 for assessment and approval.
OSHA 29 CFR 1060.17 An agency head may apply an alternate standard where deemed necessary, and shall, after consultation with employees or their representatives, including appropriate occupational safety and health committees, notify the Secretary and request approval of such alternate standards.
1960.17(a) Any request by the head of the agency for an alternate standard shall be transmitted to the Secretary.
1960.17(b) Any such request for an alternate standard shall not be approved by the Secretary unless it provides equivalent or greater protection for affected employees. Any such request shall include:
1960.17(b)(1) A statement of why the agency cannot comply with the OSHA standard or wants to adopt an alternate standard;
1960.17(b)(2) A description of the alternate standard;
1960.17(b)(3) An explanation of how the alternate standard provides equivalent or greater protection for the affected employees;
1960.17(b)(4) A description of interim protective measures afforded employees until a decision is rendered by the Secretary of Labor; and
1960.17(b)(5) A summary of written comments, if any, from interested employees, employee representatives, and occupational safety and health committees.
I would love to see this approval letter and the policy for Veterans Affairs in regards to loose-fit masks & Respitory Protection FFR’s to ensure I am protect and my Friends Employed are also Protected, and have been trying to get this via Freedom of Information Act (FOIA) and spoke to other OSHA Officers about it.
My CONCEN As far as this Brown, Derek J. is he even qualified to be the Program Administrator? Cause this Norwich Veterans Center has been in violation of not just OSHA laws but also ADA, which also offers protections to people and children with Athsma, Allergies, and other respiratory issues like Cronic Bronchitis.
Americans with Disabilities Act (ADA) doesn’t have a list it has Conditions that when meet you are protected, and for Respiratory protection it lists senarios for kids in school, who are protected and don’t even know it, nor do the teachers.
Respectfully,
Matthew Aaron Tuinstra
Stay safe, improve your overall health and stop wearing those worthless devices that pise a risk to individuals with many medical conditions that can change daily.
This is the 26th Command listed in Jewish 613 commandments, passed to them from Moses. Exodus 20:4 — King James Version (KJV 1900) “Thou shalt not make unto thee any graven image, or any likeness of any thing that is in heaven above, or that is in the earth beneath, or that is in the water under the earth: or in Exodus 20:4 — The New King James Version (NKJV)4 “You shall not make for yourself a carved image—any likeness of anything that is in heaven above, or that is in the earth beneath, or that is in the water under the earth”
Hear what the Lord says to you, people of Israel. 2 This is what the Lord says: “Do not learn the ways of the nations or be terrified by signs in the heavens, though the nations are terrified by them. For the practices of the peoples are worthless; they cut a tree out of the forest, and a craftsmanp shapes it with his chisel. They adorn it with silver and gold; they fasten it with hammer and nails so it will not totter. Like a scarecrow in a cucumber field, their idols cannot speak; they must be carried because they cannot walk. Do not fear them; they can do no harm, nor can they do any good.
”Where does this Tree worship come from? Scandinavia, Germania and Roman Paganism. The Christian adopted those in the tradition.
In the year 321 A.D., Constantine decreed, “On the venerable day of the Sun let the magistrates and people residing in cities rest, and let all workshops be closed” (Codex Justinianus lib. 3, tit. 12, 3; trans. in Philip Schaff, History of the Christian Church, Vol. 3, p. 380, note 1). This moved Sabbath to Sunday from Saturday.
Although some evidence suggests that his birth may have occurred in the spring (why would shepherds be herding in the middle of winter?), Pope Julius I chose December 25. It is commonly believed that the church chose this date in an effort to adopt and absorb the traditions of the pagan Saturnalia festival.In Scandinavia, the Norse celebrated Yule from December 21, the winter solstice, through January. In recognition of the return of the sun, In addition, members of the upper classes often celebrated the birthday of Mithra, the god of the unconquerable sun, on December 25. It was believed that Mithra, an infant god, was born of a rock. For some Romans, Mithra’s birthday was the most sacred day of the year.
St. Sylvester I. St. Sylvester I, also spelled Silvester, (born, Rome [Italy]—died 335, Rome; Western feast day December 31, Eastern feast day January 2), pope from 314 to 335, whose long pontificate saw the beginnings of the Christian Roman Empire.
Some of My comments
“Love thy God with all your heart, soul, and mind” is what Jesus said (according to KJV and most bibles of Christianity) yet we have tradition we practice in his name breaking many commands still found in the Bible, and theirs loads of Proof these were Paganism in other cultures. Why is everyone ignoring the words of the bible? Do you believe God is happy about it? Praising Him, Thy God, by doing exactly what is said DO NOT DO. Hippocrates and fake ignorant people that claim to be one thing and do differently.
In 1604, England’s King James I authorized a new translation of the Bible aimed at settling some thorny religious differences in his kingdom—and solidifying his own power. Much of the resulting translation drew on the work of the Protestant reformer William Tyndale, who had produced the first New Testament translation from Greek into English in 1525, but was executed for heresy less than a decade later. Even now, more than four centuries after its publication, the King James Bible (a.k.a. the King James Version, or simply the Authorized Version) remains the most famous Bible translation in history—and one of the most printed books ever.
In January 1604, King James convened the Hampton Court Conference, where a new English version was conceived in response to the problems of the earlier translations perceived by the Puritans, a faction of the Church of England. James gave the translators instructions intended to ensure that the new version would conform to the ecclesiology, and reflect the episcopal structure, of the Church of England and its belief in an ordained clergy. The translation was done by 6 panels of translators (47 men in all, most of whom were leading biblical scholars in England) who had the work divided up between them: the Old Testament was entrusted to three panels, the New Testament to two, and the Apocrypha to one. In common with most other translations of the period, the New Testament was translated from Greek, the Old Testament from Hebrew and Aramaic, and the Apocrypha from Greek and Latin.
More of My comments
James gave the translators instructions intended to ensure that the new version would conform, he hired 47 men to do this. Rather than get a more complete bible it actually removed what he didn’t want, what He demanded. King James is as much a Fraud as all of the Popes, they decided what is holy and whats not. Anyone who believes the Bible is complete and the perfect word of God is not only IGNORANT as heck, but likely breaking commandments because they stopped seeking TRUTH. To me christmas is the biggest lie most Christians practice, doing what is expressed NOT TO DO. The Church today is full of idiots who don’t know the bible, where it came from and whats missing from it. To me the Bible made people (STUPID) not in compliance to Gods word.
As for me, I do not OBSERVE CHRISTMAS as you do, to me it’s ANTI-CHRIST not of Christ. I follow Jesus not man. I use All the works God gives me and do not exclusively use one book that clearly REMOVED what we once were exposed to and taught. I think the Ethiopians have the most complete versions we can actually use, and should have been exposed to all our lives.
Thanks to the IDIOT Americans many Christians are actually likely to be going to hell because you can’t ask God for forgiveness of actions you had no idea were wrong, in order to repent for your sins, you must know what your sins are.
I pray you wake up and actually seek truth and stop pretending your book is the one and only, perfect, word of God. Before you can be compliant to the words of God you not only need to be exposed to them but adhear to them, practice them, and love them.
I say this out of Love, to be a seeker of truth you must compare the Bible with other books and recorded accounts of those people listed within.
Let’s sue our Med 4 TITLE 18 USC 1038 Hoax, False, & Misleading information about biological hazards. Sue any Lawyer under TITLE 18 USC 2071 Consielment, if he doesn’t allow U free speech of crimes aginst Employee Rights under OSHA 29 CFR section 19, Excutive Order #12196, OSHA 29 CFR 1910.134(f)(2), OSHA 29 CFR 1960.17, OSHA 29 CFR 1960.46(a). While the MSM & political leaders get TITLE 18 USC 35,241,242,1001,1038,2071 who convinced boss to break laws²protect employees from boss & Dr. #MAT
I love my country, and I find it very shameful our Goverment is forcing this medical terrorism in Veterans Affairs all while those Dr.’s and Nurces break the very laws concerning Respiratory Protection. I am more than qualified to be the Respiratory protection administrator for Veterans Affairs, and have been involved in it’s study, monitored programs, and training before joining the Navy and have nearly 20 years experience on the topic.
My parents also have underling medical conditions listed in OSHA 29 CFR 1910.134 Appendix (C) which exclude them from use of anu negitive pressure mask or Respiratory Device.
My ex-wife is committing child Abuse because she also has no clue why those laws were made in the first place.
If a PLHCP saw a child approximately 2 years old or younger in a department store, by law he was required to call the police for child abuse.
Their was a reason Sept 5th was used as our N95 mask awareness day in 2011, and PAPRS in 2019. To protect you from not just your Boss but also your Dr.
I have copys of OSHA’s final rule which explain ample reason from 1970’s to 1990’s why those laws were i.plemented and why every alterations must be more protective not void of them.
In 2002 Respiratory Protection was #2 on the top 10 most sited violations,as it was in 2021, and for nearly 10 years Congress debated and held many fact finding missions to learn WHY it jumped from an avg of 4th most violated to 2nd most.
We have been denied our OSHA RIGHTS under sec. 19 of the OSH Act and Excutive Order #12196 which is clearly defined under 1960.46(a) of the OSH Act sec 19 and is directly for federal agencies like Veterans Affairs.
The written respiratory protection program is required at every establishment and on hand for every employee, and trains should be given at EVERY UPDATE or CHANGE and includes who, what, when, where, and why the change is more protective utilizing NPPTL 120 tests and scenarios which prove Bacterial Filtration Efficiency.
MRSA has a 50% Mortality and is the biological agent we use for those testing and what they found was “those devices become biohazards capable of causing death and serious bodily harm to those with underling medical conditions listed in the respiratory protection questionnaire OSHA 29 CFR 1910.134 Appendix (C).
Today, and for over two years I have been requesting PAPRS so that I have the proper protection just to visit my Dr.
95% of Director’s for the building they are in charge of employee and patient safety do not have the Trai ing to be a respirator protection program administrator and have also failed to hire some like me to run it.
Ot is very much Criminal Negligence to enforce a policy in Veterans Affairs that make employees 100% likely to break those safety laws designed for your protection and also fits TITLE 19 USC 1038.
For them to hide the information violated TITLE 18 USC 2071. They have deleted many of the prior trainings and you will find many broken links on older OSHA pdf files concerning respiratory protection.
A surgical mask covers the user’s nose and mouth and provides a physical barrier to fluids and particulate materials. The surgical masks referenced in this guidance document include masks that are labeled as a surgical, laser, isolation, dental or medical procedure masks with or without a face shield.
Surgical Respirator “N95 NIOSH Certified”
A surgical respirator is fitted to the user’s face, forming a seal that provides a physical barrier to fluids, particulate materials, and aerosols. If you wish to label your device “N95 NIOSH Certified,” please refer to the (NIOSH) website at http://www.cdc.gov/niosh/npptl/resources/certpgmspt/ for information about NIOSH’s Certification Program Support for Respirator Manufacturers.
[Code of Federal Regulations][Title 21, Volume 8][CITE: 21CFR878.4040]
TITLE 21–FOOD AND DRUGSCHAPTER I–FOOD AND DRUG ADMINISTRATION DEPARTMENT OF HEALTH AND HUMAN SERVICESSUBCHAPTER H – MEDICAL DEVICESPART 878 — GENERAL AND PLASTIC SURGERY DEVICESSubpart E – Surgical DevicesSec. 878.4040 Surgical apparel.
(a) Identification. Surgical apparel are devices that are intended to be worn by operating room personnel during surgical procedures to protect both the surgical patient and the operating room personnel from transfer of microorganisms, body fluids, and particulate material. Examples include surgical caps, hoods, masks, gowns, operating room shoes and shoe covers, and isolation masks and gowns. Surgical suits and dresses, commonly known as scrub suits, are excluded.
(b) Classification.
(1) Class II (special controls) for surgical gowns and surgical masks. A surgical N95 respirator or N95 filtering facepiece respirator is not exempt if it is intended to prevent specific diseases or infections, or it is labeled or otherwise represented as filtering surgical smoke or plumes, filtering specific amounts of viruses or bacteria, reducing the amount of and/or killing viruses, bacteria, or fungi, or affecting allergenicity, or it contains coating technologies unrelated to filtration (e.g., to reduce and or kill microorganisms). Surgical N95 respirators and N95 filtering facepiece respirators are exempt from the premarket notification procedures in subpart E of part 807 of this chapter subject to § 878.9, and the following conditions for exemption:
(i) The user contacting components of the device must be demonstrated to be biocompatible.
(ii) Analysis and nonclinical testing must:
(A) Characterize flammability and be demonstrated to be appropriate for the intended environment of use; and
(B) Demonstrate the ability of the device to resist penetration by fluids, such as blood and body fluids, at a velocity consistent with the intended use of the device.(iii) NIOSH approved under its regulation.
(2) Class I (general controls) for surgical apparel other than surgicalgowns and surgical masks. The class I device is exempt from the premarket notification procedures in subpart E of part 807 of this chapter subject to § 878.9.[53 FR 23872, June 24, 1988, as amended at 65 FR 2317, Jan. 14, 2000; 83 FR 22848, May 17, 2018]
Expanded occupational use recommendation: Establish comprehensive workplace exposure standards with indicators for hazards (such as wildfire smoke) to trigger respiratory protection program requirements, including for those workplaces in which respirators would not otherwise be required.
Public use recommendation: Establish and use a standardized process for determining the public’s need for respiratory protection.
Determining the Necessary Respiratory Protective Devices
Expanded occupational use recommendation: Recommend only NIOSH-approved respirators for workers without respiratory protection programs facing inhalation hazards when other forms of control (e.g., engineering, administrative) fail to protect them.
Public use recommendation: Use hazard and risk evaluations to determine the necessary respiratory protective devices for the public.
In 2019 OSHA 1910.134 was 4 on the top most reported violations, in 2020 it rose to 3ed after being 4th for decades, and in 2021 it jumped ro 2nd. So after the pandemic we started breaking the rules.
1910.504(d)(3)(i)(B) The respirator has been stored in a breathable storage container (*e.g*., paper bag) for at least five calendar days between use and has been kept away from water or moisture;
State Plans are required to have standards and an enforcement program that are “at least as effective” as OSHA’s, but may have different or additional requirements.
Feb/Narch of 2020 I stopped talking to Dr. Kauffman because of TOTLE 18 USC 241/242 Abuse and threatening me not to talk about masks. I filed a grievance but saw no response to the offensive behavior this from Veterans Affairs lets alone a Dr.
MEMORANDUM FOR: REGIONAL ADMINISTRATORS STATE DESIGNEES.
SUBJECT: Temporary Enforcement Guidance – Healthcare Respiratory Protection Annual Fit-Testing for N95 Filtering Facepieces During the COVID-19 Outbreak
currently recommends that Health Care Providers (HCP), who are providing direct care of patients with known or suspected COVID-19, practice infection control procedures. These include engineering controls (e.g., airborne infection isolation rooms), administrative controls (e.g., cohorting patients, designated HCP), work practices (e.g., handwashing, disinfecting surfaces), and appropriate use of personal protective equipment (PPE), such as gloves, face shields or other eye protection, and gowns.
Appropriate respiratory protection is required for all healthcare personnel providing direct care of these patients
MEMORANDUM FOR: REGIONAL ADMINISTRATORS STATE PLAN DESIGNEES.
SUBJECT:
Enforcement Guidance for Respiratory Protection and the N95 Shortage Due to the Coronavirus Disease 2019 (COVID-19) Pandemic
This memorandum provides additional guidance on enforcing OSHA’s respirator standard for all workers, including HCP. In light of the essential need for adequate supplies of respirators, this memorandum will take effect immediately and remain in effect until further notice. This guidance is intended to be time-limited to the current public health crisis.
Enforcement Guidance
All employers whose employees are required to use or are permitted voluntary use of respiratory protection must continue to manage their respiratory protection programs (RPPs) in accordance with the OSHA respirator standard, and should pay close attention to shortages of N95s during the COVID-19 pandemic.[5] Paragraph (d)(1)(iii) in section 1910.134 requires such employers to identify and evaluate respiratory hazards in the workplace, and paragraph (c)(1) requires employers to develop and implement written RPPs with worksite-specific procedures and to update their written programs as necessary to reflect changes in workplace conditions that affect respirator use. CSHOs should generally refer to CPL 02-00-158, Inspection Procedures for the Respiratory Protection Standard, 6/26/2014, for further guidance.[6]
All employers whose employees are required to use or are permitted voluntary use of respiratory protection must continue to manage their respiratory protection programs (RPPs) in accordance with the OSHA respirator standard, and should pay close attention to shortages of FFRs during the COVID-19 pandemic.[7] Paragraph (d)(1)(iii) in section 1910.134 requires employers to identify and evaluate respiratory hazards in the workplace, and paragraph (c)(1) requires employers to develop and implement written RPPs with worksite-specific procedures and to update their written programs as necessary to reflect changes in workplace conditions that affect respirator use. CSHOs should generally refer to CPL 02-00-158, Inspection Procedures for the Respiratory Protection Standard, 6/26/2014, for further guidance.[8]
January 26, 2021 Denver CO Veterans Affairs violation 1910.134 (f)(2) Employers ensure tight-fitting mask and record.
May 20, 2021 Salt Lake City Utah violation 1910.134 (e)(6)(i) No referral from Dr. After EXAM by PLHCP
July 7, 2021MEMORANDUM FOR: REGIONAL ADMINISTRATORS STATE PLAN DESIGNEES
This Updated Interim Enforcement Response Plan for Coronavirus Disease 2019 (COVID-19) provides new instructions and guidance to Area Offices and Compliance Safety and Health Officers (CSHOs) for handling COVID-19-related complaints, referrals, and severe illness reports in workplaces that are not covered by the June 21, 2021, Emergency Temporary Standard for COVID-19
Although OSHA had not waived compliance with any of its requirements during the pandemic, the agency set forth temporary enforcement discretion policies that CSHOs could consider when enforcing OSHA standards, such as the Respiratory Protection standard, 29 CFR § 1910.134, and/or equivalent respiratory protection provisions of other health standards.
July 20, 3021 Gilbert AZ Violations 1910.134 (d)(1)(ii) Not NIOSH Approved , 1910.134 (e)(6)(i)(A) Limitation, & 1910.134 (g)(1)(ii) corrective lenses
Dec 2, 2021 Sputh Carolina Veterans Affairs violation of 1910.502 (h)(1) ensure 6 ft safety bubble.
Also on Dec 2, 2021 Veterans Affairs NL refused treatment while in wrong masks, and Whistleblower Sam Glover refused to take it. 1910.134 (f)(2) Tight Fit ensured by employers, 1910.134 (d)(1)(ii) wasn’t NIOSH approved, I know my limitations via 1910.134 (e)(6)(i)(A) because I understand why I’d fail 1910.134 (e)(6)(i) and another wxam would need to take place. Plus I have a beard and would require PAPR’S ro get any respiratory protection. The Veterans Affairs patient advocate refused to take my claim aswell.
December 16, 2021 Wyoming Michigan Veterans Affairs violation 1910.502 (f)(2)(i) which is a violation of 1910.134 and (several possibilities all mask related)
December 17, 2021 Phoenix AZ Veterans Affairs violation 1910.504 (d)(3)(i)(B) paper bag for greater than 5 days.
March 4, 2022 I was again refused treatment from Veterans Affairs NL with a letter from the Director Mark Bielawski APRN, and he could not verify any laws which prevent my treatment. Again this Whistleblower reported to Sam Glover and the Veterans Affairs Patient advocate no actiona were takes to resolve any issues.
March 7, 2022 Baltimore Veterans Affairs violations 1910.134 (f)(2) employers ensure tight fitt masks, 1910.502 (f)(2)(i) another 1910.134 violation & more.
April 14, 2022 Cincinnati OH Veterans Affairs violation 1910.134 (f)(2) employers ensure employees use tight fitting masks.
The meeting analyzed the criminal mercenary bands organized by the CIA, the NATO, and permitted, encouraged and financed by reactionary governments in the Middle East that continue killing men, women, children and indigenous people in massive form, that have brought a forced migration full of hunger, poverty, discrimination and without some hope for survival.
It was very wonderful to chat, I have gathered lots of data on this topic.
“Although OSHA had not waived compliance with any of its requirements during the pandemic, the agency set forth temporary enforcement discretion policies that CSHOs could consider when enforcing OSHA standards, such as the Respiratory Protection standard, 29 CFR § 1910.134, and/or equivalent respiratory protection provisions of other health standards.”
This is some of the data I’ve still got access to, other information like 1918 Pandemic articles Co-Authored by Fauci himself was removed from PUBMED.GOV in 2020.
On Dec 2nd 2021 I was refused Medical treatment via Veterans Affairs. At this point in Time it had been 2 weeks since the Veterans Affairs Commissioner reported any positive results of SARS-COV, the total who did test positive was 76 Staff and 74 patrons where 5 patrons died with 2 staff members. I have been keeping track.
I know the laws, was an instructor for OSHA 10 & 30, HACCP, and Emergency Medical Assistance Team on Submarines for nearly 15 years
I made a Whistleblower claim to the Veterans Whistleblower online to report the “1910.134(d)(1)(ii) The employer shall select a NIOSH-certified respirator. The respirator shall be used in compliance with the conditions of its certification” via Whistleblower Protection (OAWP) on 3/11/2022. Before that I reported the VA wearing the wrong masks in Dec 2021 after being refused medical treatment, only for Sam Glover from PA to refuse it, when clearly it was a violation, Sam Glover refused to take my claim. case referral 22-NorwichCT-18500. Other numbers 22-WestHavenCT-18503 22-WestHavenCT-18926
In 2019 OSHA 1910.134 was 4 on the top most reported violations, in 2020 it rose to 3ed after being 4th for decades, and in 2021 it jumped ro 2nd. So after the pandemic we started breaking the rules.
**Listed in PCD order** 1904.29(b)(1) *What do I need to do to complete the OSHA 300 Log?* You must enter information about your business at the top of the OSHA 300 Log, enter a one or two line description for each recordable injury or illness, and summarize this information on the OSHA 300-A at the end of the year
1904.29(b)(2) *What do I need to do to complete the OSHA 301 Incident Report?* You must complete an OSHA 301 Incident Report form, or an equivalent form, for each recordable injury or illness entered on the OSHA 300 Log.
1904.29(b)(3) *How quickly must each injury or illness be recorded?* You must enter each recordable injury or illness on the OSHA 300 Log and 301 Incident Report within seven (7) calendar days of receiving information that a recordable injury or illness has occurred.
1904.29(b)(7)(v) Needlestick injuries and cuts from sharp objects that are contaminated with another person’s blood or other potentially infectious material (see §1904.8 for definitions); and
1904.4(a)-(X3) *Basic requirement*. Each employer required by this part to keep records of fatalities, injuries, and illnesses must record each fatality, injury and illness that
1904.7(b)(3) ***How do I record a work-related injury or illness that results in days away from work?*** When an injury or illness involves one or more days away from work, you must record the injury or illness on the OSHA 300 Log with a check mark in the space for cases involving days away and an entry of the number of calendar days away from work in the number of days column. If the employee is out for an extended period of time, you must enter an estimate of the days that the employee will be away, and update the day count when the actual number of days is known.
1910.132(d)(1)(i) Select, and have each affected employee use, the types of PPE that will protect the affected employee from the hazards identified in the hazard assessment
1910.134(a)(2) A respirator shall be provided to each employee when such equipment is necessary to protect the health of such employee. The employer shall provide the respirators which are applicable and suitable for the purpose intended. The employer shall be responsible for the establishment and maintenance of a respiratory protection program, which shall include the requirements outlined in paragraph (c) of this section. The program shall cover each employee required by this section to use a respirator.
1910.134(d)(1)(ii) The employer shall select a NIOSH-certified respirator. The respirator shall be used in compliance with the conditions of its certification.
1910.134(e)(1)-(X2) General. The employer shall provide a medical evaluation to determine the employee’s ability to use a respirator, before the employee is fit tested or required to use the respirator in the workplace. The employer may discontinue an employee’s medical evaluations when the employee is no longer required to use a respirator.
1910.134(e)(6)(i) Obtain a written recommendation regarding the employee’s ability to use the respirator from the PLHCP. The recommendation shall provide only the following information:
1910.134(e)(6)(i)(A) Any limitations on respirator use related to the medical condition of the employee, or relating to the workplace conditions in which the respirator will be used, including whether or not the employee is medically able to use the respirator.
1910.134(f)(2)-(X4) The employer shall ensure that an employee using a tight-fitting facepiece respirator is fit tested prior to initial use of the respirator, whenever a different respirator facepiece (size, style, model or make) is used, and at least annually thereafter.
1910.134(g)(1)(ii) If an employee wears corrective glasses or goggles or other personal protective equipment, the employer shall ensure that such equipment is worn in a manner that does not interfere with the seal of the facepiece to the face of the user.
1910.134(k)(5) Retraining shall be administered annually, and when the following situations occur.
1910.134(m)(2)(ii) The employer shall establish a record of the qualitative and quantitative fit tests administered to an employee including.
1910.502(c)(5) The employer must seek the input and involvement of non-managerial employees and their representatives, if any, in the hazard assessment and the development and implementation of the COVID-19 plan.
1910.502(f)(2)(i)-(X2) A respirator to each employee and ensure that it is provided and used in accordance with § 1910.134 and
1910.502(h)(1)-(X4) The employer must ensure that each employee is separated from all other people by at least 6 feet when indoors unless the employer can demonstrate that such physical distancing is not feasible for a specific activity (*e.g.*, hands-on medical care). This provision does not apply to momentary exposure while people are in movement (*e.g.*, passing in hallways or aisles).
1910.502(j)(2)(i) Clean high-touch surfaces and equipment at least once a day, following manufacturers’ instructions for application of cleaners; and
1910.502(l)(3)(i)(A)-(X3) Notify each employee who was not wearing a respirator and any other required PPE and has been in close contact with that person in the workplace. The notification must state the fact that the employee was in close contact with someone with COVID-19 along with the date(s) that contact occurred.
1910.502(l)(5)(iii)(A) The employer must continue to provide the benefits to which the employee is normally entitled and must also pay the employee the same regular pay the employee would have received had the employee not been absent from work, up to $1,400 per week, until the employee meets the return to work criteria specified in paragraph (l)(4)(iii) or (l)(6) of this section.
1910.502(n)(1)(ix) Available sick leave policies, any COVID-19-related benefits to which the employee may be entitled under applicable federal, state, or local laws, and other supportive policies and practices (*e.g.*, telework, flexible hours);
1910.502(q)(2)(ii)(A) The COVID-19 log must contain, for each instance, the employee’s name, one form of contact information, occupation, location where the employee worked, the date of the employee’s last day at the workplace, the date of the positive test for, or diagnosis of, COVID-19, and the date the employee first had one or more COVID-19 symptoms, if any were experienced.
1910.502(r)(1)(i) Each work-related COVID-19 fatality within 8 hours of the employer learning about the fatality.
1910.502(r)(1)(ii) When reporting COVID-19 fatalities and in-patient hospitalizations to OSHA in accordance with paragraph (r)(1) of this section, the employer must follow the requirements in 29 CFR 1904.39, except for 29 CFR 1904.39(a)(1) and (2) and (b)(6).
1910.504(d)(3)(i)(B) The respirator has been stored in a breathable storage container (*e.g*., paper bag) for at least five calendar days between use and has been kept away from water or moisture;
1960.66(b) Except as modified by this subpart, Federal agency injury and illness recording and reporting requirements shall comply with the requirements under 29 CFR Part 1904, subparts C, D, E, and G, except that the definition of “establishment” found in 29 CFR 1960.2(h) will remain applicable to Federal agencies.
I want you to join my group on MeWe or go HERE for misinformation or go to CNN for hoax information.
Are you doing it properly?
Study for OSHA shows Employers in 2020 who had 5A1 Citations for Wilful Neglect of OSHA 29 CFR 1910.134 moved from 4th most common safety violation to 3ed most reported safety violation.
January 8, 2021 U.S. Department of Labor’s OSHA Announces $3,930,381 In Coronavirus Violations OSHA inspections have resulted in the agency citing employers for violations, including failures to:
Implement a written respiratory protection program;
Provide a medical evaluation, respirator fit test, training on the proper use of a respirator and personal protective equipment;
Report an injury, illness or fatality;
Record an injury or illness on OSHA recordkeeping forms; and
5. Comply with the General Duty Clause of the Occupational Safety and Health Act of 1970.
Inspections with COVID-19 related Violations if you look to the far right, you will see hundreds on OSHA 29 CFR 1910.134 5A1 Wilful Neglect violations. In 2020 their was 60,000 plus inspections and this number gets lower every year.
OMG here we have Microfiber Masks that did not pass any of the 510(k) reviews and would fail the NPPTL testing for NIOSH certification for use in hospitals and industries. This KN95, shown with GB2626 2019, is a product of China and those masks failed NIOSH certification because it didn’t allow proper airflow and due to Microfiber being a perfect breeding ground for biological hazards it is not responsible to buy this product, it’s a danger to you and others when not used properly and as a disposable single-use item. https://www.oprahdaily.com/life/health/g38960590/best-kn9product
“masking is a critical public health tool for preventing the spread of Covid-19,” and “any mask is better than no mask,”
False Both those statements are false. Masks are not at all critical in healthcare, PPE is the least effective form of protection out of all the cross containment prevention measures, and a bad mask can be more dangerous than using a mask, it could already be infected and doesn’t come sterilized**.
The agency says loosely woven cloth masks provide the least protection, layered finely woven products offer more protection, well-fitting disposable surgical masks and KN95s offer even more protection, and well-fitting NIOSH-approved respirators (including N95s) offer the highest level of protection.
False KN95 and well fitted surgical masks do not offer more protection, especially if their not single-use, their are levels of protection from extensive study, N, R, and P are for Not resistant, water and oil resistant, water and oil protection, as well as 95%, 99%, and 100% filter efficiency, this does not include Bacterial protection efficiency (BPE)
Order of efficiency of FFR’s Least effective to most effective SM’s (Surgical Masks) N95 N99 N100 R95 R99 R100 P95 P99 P100 Half face elastomeric respirator Air Supplied respirators or PAPR’s
So the best protection is with Air Supplied or PAPR’s
The N95 and KN95 respirator masks are largely the same, explains Niket Sonpal, MD, an internist in New York City.
False those masks are 100% completely different and KN95’s are a danger to people who already have underlying healtissues like; COPD, athsma, lung cancer or recovering, influenza, Bronchitis, Tuberculosis, Pneumonia, allergies, or when exposed to some chemicals that absorbed into the cloth, as listed in OSHA 29 CFR 1910.134 Appendix (C) with your ANSI/ASSE Z88.2 – 2015 Practices for Respiratory Protection and Z88.6 Respiratory use Qualification exam.
NOTE: Niket Sonpal violated TITLE 18 USC 1038, and is on Oprah’s news website. violation is 5 to 20 years in prison and/or up to $200,000 in fines.
“Both masks are rated to capture 95 percent of tiny particles (0.3 micron particles),” he says. “The difference between them is considered to be the pressure drop while inhaling, but this is primarily to protect healthcare workers.
FALSE they knew this wouldn’t pass the FDA 510(k) review because it is a negitive pleasure loose-fitting mask, and it’s made out of thick Microfiber (breeding ground for biological hazards) P.S. SM’s and FFR’s like N95’s are tested with 0.1-micron latex spheres not 0.3 as listed on the Fake Oprah’s news website.
With this in mind, a KN95 mask is your best bet for the most protection against Covid-19 during day-to-day activities.
False masks are the lease effect measures to prevent the spread of biohazards. The most effective is PAPR’s and other Air Supplied Respiratory Protection.
Finally, adjust the metal nose clip to the shape of your nose and adjust fit as necessary to reduce airflow around the mask.
DANGER necessary to reduce airflow, are you trying to cause hypoxia? Which also is rather deadly and has the same symptoms as Coronavirus, Colds, Flu, SARS, and Pneumonia.
7. Be sure to change out your mask at least every few wears. The CDC says healthcare workers can wear an N95 mask up to five times, says Sonpal.
False it is recommended to be disposable, single-use just as the SM’s and FFR N95’s. It wasn’t ever recommended to use more than once untill.the Pandemic, and their is a list of cleaning agents healthcare can use up to 3 times between patients to conserve on supplies when running low, if it’s not running low it’s single use to prevent spreading biohazards from patient #1 and giving to patient #2 the HAI.
Risks to Health
In the table below, FDA has identified the risks to health generally associated with the use of the surgical masks addressed in this document. The information we recommend you include in your 510(k) to address these identified risks are given in this guidance document, as shown in the table below. We recommend that you conduct a risk analysis, before submitting your 510(k), to identify any other risks specific to your device. The 510(k) should describe the risk analysis method. If you elect to use an alternative approach to address a particular risk identified in this document, or have identified risks additional to those in this document, you should provide sufficient detail to support the approach you have used to address that risk.
Identified risk
Inadequate fluid resistance
Inadequate barrier for bacteria
Inadequate air exchange (differential pressure)
Flammability
Inadequate respiratory barrier for bacteria
NIOSH certification, Surgical masks include parts that have prolonged contact with intact skin. We recommend that you evaluate the biocompatibility of the materials in these parts as described in the standard ISO-10993, “Biological Evaluation of Medical Devices Part 1: Evaluation and Testing” for limited contact devices, contacting intact skin. We also recommend that you document the results in your design history file as a part of the Quality Systems Requirements (21 CFR 820.30). You should select tests appropriate for the duration and level of contact with your device. If identical materials are used in a predicate device with the same type and duration of skin contact, you may identify the predicate device in lieu of performing biocompatibility testing.
“Filtration Efficiency For surgical masks that are not NIOSH certified N95 Respirators, we recommend that you evaluate filter efficiency performance and bacterial filtration efficiency. For surgical masks that are NIOSH certified N95 Respirators, you may submit your NIOSH certification number in lieu of this information.
Particulate Filtration Efficiency
We recommend that you conduct a particle challenge study using 0.1-Micron Polystyrene Latex Spheres. This in vitro test challenges the mask with unneutralized 0.1-micron polystyrene latex spheres and measures penetration. The use of latex spheres provides an appropriately rigorous test for evaluating a submicron efficiency performance (ASTM F 1215-89 Standard Test Method for Determining the Initial Efficiency of Flatsheet Filter Medium in an Airflow Using Latex Spheres.).
Bacterial Filtration Efficiency
Bacterial Filtration Efficiency (BFE) is a measure of the ability of the mask’s material to prevent the passage of aerosolized bacteria. BFE is expressed in the percentage of a known quantity that does not pass the mask material at a given aerosol flow rate. We recommend that you evaluate the BFE of your device using one of the test methods or standards listed below.
Bacterial Penetration (aerosol filtration) – Mil- M369454C, Military Specifications: Surgical Mask, disposable (June 12, 1975). Modified Greene and Vesley Method: Method for evaluation of bacterial filtration efficiency of surgical masks. J Bacteriol 83:663-667. (1962). ASTM F2101-01 Standard Test Method for Evaluating the Bacterial Filtration Efficiency (BFE) of surgical masks using a Biological Aerosol of Staphylococcus aureus. Back to the top”
“Abstract Respiratory syncytial virus (RSV) infections in hospitalized children were identified by indirect fluorescent antibody technique. Patients with RSV infections were assigned to one of two isolation categories. In one category, the health care workers entering the child’s room did not wear masks and goggles; in the other category, the workers did wear masks and goggles. The RSV illness rate in health care workers using masks and goggles was 5%, but the rate for those using masks and not goggles was 61%. In the no mask/goggles group, the RSV illness rates in the health care workers correlated directly with the number of exposures. In this modest study, the use of masks and goggles was associated with a significant reduction of RSV illnesses in pediatric health care workers.” https://thumbs.gfycat.com/ClearReflectingEuropeanpolecat-mobile.jpg#h=360w=640
“At Denver Children’s Hospital, Murphy et al looked at the effectiveness of gowns and masks in preventing RSV infection in pediatric hospital personnel 6. They found that gowning and masking did not increase personal protection against RSV infection above that which was provided by the usual hand-washing routine 6. We at UCLA and Hall and her colleagues were both aware that conjunctional surfaces could be a site for RSV infections [7–10]. Our group compared standard isolation precautions with standard procedures supplemented by the use of masks and goggles. Among the healthcare workers who wore masks and goggles for clinical care, the infection rate was 5% compared with 61% among the healthcare workers who did not wear masks and goggles “
26,976 DEATHS 277 MORE DEATHS IN JUST 7 DAYS 219,865 SERIOUS INJURIES 2,564 MORE INJURIES IN JUST 7 DAYS
MISCARRIAGES 4,496 HEART ATTACKS 13,819 MYO/PERICARDITIS 38,605 PERMANENTLY DISABLED 50,100 LIFE THREATENING 30,293 SHINGLES 13,413 AND THE LIST GOES ON
“December 20, 2017 Mr. John Boren 3633 Wareham Drive Thompsons Station, TN 37179
Dear Mr. Boren:
Thank you for your letter to the Occupational Safety and Health Administration (OSHA). Your letter has been referred to the Directorate of Enforcement Programs for an answer to your question. Your letter requested clarification of OSHA’s Respiratory Protection Standard, 29 CFR 1910.134, pertaining to the voluntary use of surgical masks. This letter constitutes OSHA’s interpretation only of the requirements discussed herein, and may not be applicable to any questions not delineated within your original correspondence. Your paraphrased question and our response are below.
Question: Is it permissible to allow surgical masks to be worn on a voluntary basis when respiratory protection is not required to meet any OSHA standards? And if so, is it permissible for employers to provide surgical masks for voluntary use?
Response: Yes. The employer may allow the voluntary use of surgical masks even where an exposure assessment shows respirator use is not required and the employer may provide surgical masks for voluntary use. However, surgical masks may not be used in lieu of required respiratory protection. Surgical masks are not considered respirators by OSHA and, as such, are not covered by 29 CFR 1910.134. They are fluid resistant, disposable, and loose-fitting protection that create a physical barrier between the mouth and nose of the wearer and potential contaminants in the immediate environment. They are commonly used in health care settings for the protection of the patient and they are also often used to prevent splashes from contacting the face of the wearer. However, surgical masks do not seal tightly to the wearer’s face, nor do they provide a reliable level of protection from inhaling smaller airborne particles.
If the hazard to which your employees are exposed to is a combination of splashes and respirable contaminants, your company may want to consider NIOSH approved surgical N95 respirators which also are cleared by the Food and Drug Administration (FDA) for use as a surgical mask. Surgical N95s are filtering facepiece respirators equipped with spray- or splash-resistant facemask material on the outside to protect the wearer from splashes. Regardless of which type is used, the employees should be informed on the different varieties and their unique set of cautions, limitations, and restrictions of use. This information will facilitate employee involvement in the respirator program and/or the overall safety and health program.
Please be aware that the Tennessee Department of Labor and Workforce Development operates its own occupational safety and health program under an OSHA-approved State Plan. The Tennessee Occupational Safety and Health Administration (TOSHA) adopts and enforces standards and investigates safety and health concerns in workplaces throughout the state. State Plans are required to have standards and an enforcement program that are “at least as effective” as OSHA’s, but may have different or additional requirements. Please contact TOSHA directly at the address below, for further information and to discuss your specific compliance issue:
Tennessee Department of Labor and Workforce Development
Thank you for your interest in occupational safety and health. We hope you find this information helpful. OSHA’s requirements are set by statute, standards, and regulations. Our letters of interpretation do not create new or additional requirements but rather explain these requirements and how they apply to particular circumstances. This letter constitutes OSHA’s interpretation of the requirements discussed. From time to time, letters are affected when the agency updates a standard, a legal decision impacts a standard, or changes in technology affect the interpretation. To assure that you are using the correct information and guidance, please consult OSHA’s website at http://www.osha.gov. If you have further questions, please feel free to contact the Office of Health Enforcement at (202) 693-2190.
Sincerely,
Thomas Galassi, Director Directorate of Enforcement Programs
March 14, 2020 MEMORANDUM FOR: REGIONAL ADMINISTRATORS STATE DESIGNEES
THROUGH: AMANDA EDENS, Deputy Assistant Secretary FROM: PATRICK J. KAPUST, Acting Director Directorate of Enforcement Programs
SUBJECT: Temporary Enforcement Guidance – Healthcare Respiratory Protection Annual Fit-Testing for N95 Filtering Facepieces During the COVID-19 Outbreak
This memorandum provides temporary enforcement guidance to Compliance Safety and Health Officers for enforcing the Respiratory Protection standard, 29 CFR § 1910.134, with regard to supply shortages of N95 filtering facepiece respirators due to the COVID-19 outbreak. The Respiratory Protection standard has specific requirements, including a written program, medical evaluation, fit-testing, and training, that employers must follow to ensure workers are provided and are properly using appropriate respiratory protection when necessary to protect their health.1 On March 11, 2020, the President directed the Department of [Health and Human services to “take all appropriate and necessary steps with respect to general use respirators to facilitate their emergency use by healthcare personnel in healthcare facilities and elsewhere,” and he directed the Department of Labor to “consider all appropriate and necessary steps to increase the availability of respirators.”] In light of the Presidential Memorandum, OSHA is providing this temporary guidance for 29 CFR § 1910.134, regarding required annual fit-testing (paragraph (f)(2)), which is to take effect from the date of this memorandum and remain in effect until further notice.
The Centers for Disease Control and Prevention (CDC) currently recommends that Health Care Providers (HCP), who are providing direct care of patients with known or suspected COVID-19, practice infection control procedures. These include engineering controls (e.g., airborne infection isolation rooms), administrative controls (e.g., cohorting patients, designated HCP), work practices (e.g., handwashing, disinfecting surfaces), and appropriate use of personal protective equipment (PPE), such as gloves, face shields or other eye protection, and gowns.
Appropriate respiratory protection is required for all healthcare personnel providing direct care of these patients. For additional guidance, see COVID-19 Hospital Preparedness Assessment Tool, [https://www.cdc.gov/coronavirus/2019-ncov/hcp/hcp-hospital-checklist.html][https_www.cdc.gov_coronavirus_2019-ncov_hcp_hcp-hospital-checklist.html].
OSHA recommends HCP employers follow existing CDC guidelines, including taking measures to conserve supplies of these respirators while safeguarding HCP. One such measure is that healthcare employers may provide HCP with another respirator of equal or higher protection, such as N99 or N100 filtering facepieces, reusable elastomeric respirators with appropriate filters or cartridges, or powered air purifying respirators (PAPR). Another measure is that healthcare employers may change the method of fit testing from a destructive method (i.e., quantitative) to a non-destructive method (i.e., qualitative). For filtering facepiece respirators, qualitative and quantitative fit-testing methods are both effective at determining whether the respirator fits properly. See 29 CFR § 1910.134, Appendix A, [Fit Testing Procedures][].2 The fitted respirator can then be safely used for work tasks that require respiratory protection. For additional guidance, see Strategies for Optimizing the Supply of N95 Respirators, [https://www.cdc.gov/coronavirus/2019-ncov/hcp/respirator-supply-strategies.html][https_www.cdc.gov_coronavirus_2019-ncov_hcp_respirator-supply-strategies.html].3
OSHA field offices shall exercise enforcement discretion concerning the annual fit testing requirement, 29 CFR § 1910.134(f)(2), as long as employers:
Make a good-faith effort to comply with 29 CFR § 1910.134;
Use only NIOSH-certified respirators;
Implement CDC and OSHA strategies for optimizing the supply of N95 filtering facepiece respirators and prioritizing their use, as discussed above;
Perform initial fit tests for each HCP with the same model, style, and size respirator that the worker will be required to wear for protection against COVID-19 (initial fit testing is essential to determine if the respirator properly fits the worker and is capable of providing the expected level of protection);
Inform workers that the employer is temporarily suspending the annual fit testing of N95 filtering facepiece respirators to preserve and prioritize the supply of respirators for use in situations where they are required to be worn;
Explain to workers the importance of performing a user seal check (i.e., a fit check) at each donning to make sure they are getting an adequate seal from their respirator, in accordance with the procedures outlined in 29 CFR § 1910.134, Appendix B-1, User Seal Check Procedures.4 See also, OSHA tutorial videos (English, Spanish).5
Conduct a fit test if they observe visual changes in the employee’s physical condition that could affect respirator fit (e.g., facial scarring, dental changes, cosmetic surgery, or obvious changes in body weight) and explain to workers that, if their face shape has changed since their last fit test, they may no longer be getting a good facial seal with the respirator and, thus, are not being adequately protected; and,
Remind workers that they should inform their supervisor or their respirator program administrator if the integrity and/or fit of their N95 filtering facepiece respirator is compromised.
NOTE: Workers should visually inspect the N95 respirator to determine if the structural and functional integrity of the respirator has been compromised. Over time, components such as the straps, nose bridge, and nose foam material may degrade, which can affect the quality of the fit and seal. If the structural and functional integrity of any part of the respirator is compromised, or if a successful user seal check cannot be performed, discard the respirator and try another respirator.
Where the use of respiratory protection is required and an employer fails to comply with any other requirements, such as initial fit testing, maintenance, care, and training in the Respiratory Protection standard, cite the applicable section(s) of 29 CFR § 1910.134.
To emphasize, this is an enforcement discretion policy, beginning from the date of this memorandum, and applicable where respirators are needed to protect HCP during the COVID-19 outbreak. This temporary enforcement discretion policy will no longer apply upon notification. If you have any questions regarding this policy, please contact Dr. Dionne Williams at (202) 693-2140.
April 3, 2020 MEMORANDUM FOR: REGIONAL ADMINISTRATORS STATE PLAN DESIGNEES
THROUGH: AMANDA EDENS, Deputy Assistant Secretary FROM: PATRICK J. KAPUST, Acting Director Directorate of Enforcement Programs
SUBJECT: Enforcement Guidance for Respiratory Protection and the N95 Shortage Due to the Coronavirus Disease 2019 (COVID-19) Pandemic
This memorandum provides interim guidance to Compliance Safety and Health Officers (CSHOs) for enforcing the Respiratory Protection standard, 29 CFR § 1910.134, and certain other health standards, with regard to supply shortages of disposable N95 filtering facepiece respirators. Specifically, it outlines enforcement discretion to permit the extended use and reuse of respirators, as well as the use of respirators that are beyond their manufacturer’s recommended shelf life (sometimes referred to as “expired”). This guidance applies in all industries, including workplaces in which:
Healthcare personnel (HCP) are exposed to patients with suspected or confirmed coronavirus disease 2019 (COVID-19) and other sources of SARS-CoV-2 (the virus that causes COVID-19).
Protection of workers exposed to other respiratory hazards is impacted by the shortage resulting from the response to the COVID-19 pandemic. Such workplace respiratory hazards may be covered by one or more substance-specific health standards.
Our previous memorandum, Temporary Enforcement Guidance – Healthcare Respiratory Protection Annual Fit-Testing for N95 Filtering Facepieces During the COVID-19 Outbreak, issued on March 14, 2020, provided temporary guidance for 29 CFR § 1910.134, regarding required annual fit testing of HCP.1 This memorandum provides additional guidance on enforcing OSHA’s respirator standard for all workers, including HCP. In light of the essential need for adequate supplies of respirators, this memorandum will take effect immediately and remain in effect until further notice. This guidance is intended to be time-limited to the current public health crisis. Please frequently check OSHA’s webpage at www.osha.gov/coronavirus for updates.
Background
The COVID-19 outbreak, which the World Health Organization recently declared a global pandemic, has created an increased demand for N95 filtering facepiece respirators, limiting availability for use in protecting workers in healthcare and emergency response from exposure to the virus. As a result, the President directed the Secretary of Labor to “[consider] all appropriate and necessary steps to increase the availability of respirators.”2
The Food and Drug Administration (FDA) also issued an Emergency Use Authorization (EUA) letter permitting National Institute for Occupational Safety and Health (NIOSH)-approved, disposable filtering facepiece respirators, including those that were NIOSH-approved but have since passed the manufacturer’s recommended shelf life, to be used in healthcare settings to mitigate further transmission of SARS-CoV-2.3
During N95 filtering facepiece respirator (FFR) shortages, the federal government advises that specific N95 FFRs that are beyond their manufacturer’s recommended shelf life will provide greater protection than surgical masks (i.e., facemasks, other than surgical N95s; see below) or non-NIOSH-approved masks (e.g., homemade masks or improvised mouth and nose covers, such as bandanas). NIOSH has tested a sample of N95 FFRs that are beyond their manufacturer’s recommended shelf life from facilities across the United States and determined that certain N95 models continue to protect against the hazards for which they would ordinarily be appropriate (for N95 FFRs, this means they are still expected to filter out 95% of particles of the most penetrating particle size, or 0.3 µm). However, the Centers for Disease Control and Prevention (CDC) and NIOSH have recommended that expired N95 FFRs be used only as outlined in their Strategies for Optimizing the Supply of N95 Respirators.4 For more information, see www.cdc.gov/coronavirus/2019-ncov/release-stockpiled-N95.html.
Enforcement Guidance
All employers whose employees are required to use or are permitted voluntary use of respiratory protection must continue to manage their respiratory protection programs (RPPs) in accordance with the OSHA respirator standard, and should pay close attention to shortages of N95s during the COVID-19 pandemic.5 Paragraph (d)(1)(iii) in section 1910.134 requires such employers to identify and evaluate respiratory hazards in the workplace, and paragraph (c)(1) requires employers to develop and implement written RPPs with worksite-specific procedures and to update their written programs as necessary to reflect changes in workplace conditions that affect respirator use. CSHOs should generally refer to CPL 02-00-158, Inspection Procedures for the Respiratory Protection Standard, 6/26/2014, for further guidance.6
Due to the impact on workplace conditions caused by limited supplies of N95 FFRs, all employers should reassess their engineering controls, work practices, and administrative controls to identify any changes they can make to decrease the need for N95 respirators. Employers should, for example, consider whether it is possible to increase the use of wet methods or portable local exhaust systems or to move operations outdoors. In some instances, an employer may also consider taking steps to temporarily suspend certain non-essential operations.
If respiratory protection must be used, employers may consider use of alternative classes of respirators that provide equal or greater protection compared to an N95 FFR, such as NIOSH-approved, non-disposable, elastomeric respirators or powered, air-purifying respirators (PAPRs). Other filtering facepiece respirators, such as N99, N100, R95, R99, R100, P95, P99, and P100, are also permissible alternatives for those who are unable to obtain N95 FFRs. However, per 29 CFR § 1910.134(d)(1)(ii), when considering N95 alternatives, check to ensure that they are NIOSH-approved, at www.cdc.gov/niosh/npptl/topics/respirators/disp_part/default.html. When these alternatives are not available, or where their use creates additional safety or health hazards, employers may consider the extended use or reuse of N95 FFRs or use of N95 FFRs that were NIOSH-approved but have since passed the manufacturer’s recommended shelf life.
The following specific enforcement guidance is provided for CSHOs inspecting workplaces where workers are using N95 FFRs.
All employers:
Extended use or reuse of N95s: In the event extended use or reuse of N95 FFRs becomes necessary, the same worker is permitted to extend use of or reuse the respirator, as long as the respirator maintains its structural and functional integrity and the filter material is not physically damaged, soiled, or contaminated (e.g., with blood, oil, paint).7 Employers must address in their written RPPs the circumstances under which a disposable respirator will be considered contaminated and not available for extended use or reuse. Extended use is preferred over reuse due to contact transmission risk associated with donning/doffing during reuse. When respirators are being re-used, employers should pay particular attention to workers’ proper storage of the FFRs in between periods of reuse.
Users should perform a user seal check each time they don a respirator and should not use a respirator on which they cannot perform a successful user seal check. See 29 CFR § 1910.134, Appendix B-1, User Seal Check Procedures.8
Employers should train workers to understand that if the structural and functional integrity of any part of the respirator is compromised, it should be discarded, and that if a successful user seal check cannot be performed, another respirator should be tried to achieve a successful user seal check.
If reuse of respirators is necessary, an appropriate sequence for donning/doffing procedures should be used to prevent contamination, and training needs to address appropriate donning/doffing procedures. Seewww.cdc.gov/niosh/npptl/pdfs/PPE-Sequence-508.pdf.
Use of expired N95s: In the event that N95s are not available and the employer has shown a good faith effort to acquire the respirators or to use alternative options, as outlined below, CSHOs should exercise enforcement discretion for the use of N95 FFRs beyond the manufacturer’s recommended shelf life, including surgical N95s.9
Purchasers and users of personal protective equipment should not co-mingle products that are past their manufacturer’s recommended shelf life (i.e., expired) with items that are within their shelf life.
Employers should visually inspect, or ensure that workers visually inspect, the N95 FFRs to determine if the structural and functional integrity of the respirator has been compromised. Over time, components such as the straps, nose bridge, and nose foam material may degrade, which can affect the quality of the fit and seal.
Where an employer has expired N95s available from their own stored cache (i.e., not from the U.S. Strategic National Stockpile), the employer should seek assistance from the respirator manufacturer or independent lab regarding testing of those stored respirators prior to use.
Healthcare employers only:
Expired N95s generally must not be used when HCP:
Perform surgical procedures on patients infected with, or potentially infected with, SARS-CoV-2, or perform or are present for procedures expected to generate aerosols or procedures where respiratory secretions are likely to be poorly controlled (e.g., cardiopulmonary resuscitation, intubation, extubation, bronchoscopy, nebulizer therapy, sputum induction).
In accordance with CDC guidance for optimizing the supply of respirators, employers should prioritize the use of N95 respirators by activity type. When HCP perform or are present for aerosol-generating procedures or procedures where respiratory secretions are likely to be poorly controlled, use respirators (including N95 FFRs; other FFRs; non-disposable, elastomeric respirators; and PAPRs) that are still within their manufacturer’s recommended shelf life, if available, before using respirators that are beyond their manufacturer’s recommended shelf life. See www.cdc.gov/coronavirus/2019-ncov/hcp/respirators-strategy/contingency-capacity-strategies.html. The CDC guidance also addresses scenarios in which other crisis standards of care may need to be considered, but this enforcement guidance is not intended to cover those scenarios.
As mentioned above, the FDA has concluded that respirators approved by NIOSH, but not currently meeting the FDA’s requirements, may be protective against SARS-CoV-2. The FDA is providing a list of authorized emergency-use respirators for HCP. Healthcare employers may view the list of approved respirators, and respirator manufacturers and stockpile managers may find information about how to obtain approval for expired respirators, at: www.fda.gov/media/135763/download and http://www.fda.gov/media/135921/download.
Citation guidance:
OSHA will, on a case-by-case basis, exercise enforcement discretion when considering issuing citations under 29 CFR § 1910.134(d) and/or the equivalent respiratory protection provisions of other health standards in cases where:
The employer has made a good faith effort to obtain other alternative filtering facepiece respirators, reusable elastomeric respirators, or PAPRs appropriate to protect workers;
Surgical masks and eye protection (e.g., face shields, goggles) were provided as an interim measure to protect against splashes and large droplets (note: surgical masks are not respirators and do not provide protection against aerosol-generating procedures); and
Other feasible measures, such as using partitions, restricting access, cohorting patients (healthcare), or using other engineering controls, work practices, or administrative controls that reduce the need for respiratory protection, were implemented to protect employees.
Where the above efforts are absent and respiratory protection use is required, or voluntary use is permitted, and an employer fails to comply with fit testing, maintenance, care, and training requirements, cite the applicable provision(s) of 29 CFR § 1910.134 and/or other applicable expanded health standards as serious violations. If you have any questions regarding this policy, please contact the Directorate of Enforcement Programs at (202) 693-2190.
9 Surgical N95s are NIOSH-approved N95 FFRs that are also certified by the FDA for use as a surgical mask. Surgical N95s are normally tested for fluid resistance and flammability. These requirements were not evaluated as part of the NIOSH shelf life testing discussed in this memorandum. CDC/NIOSH does not recommend using N95s beyond the manufacturer-designated shelf life in surgical settings. Back to Text[Back to Text 8]

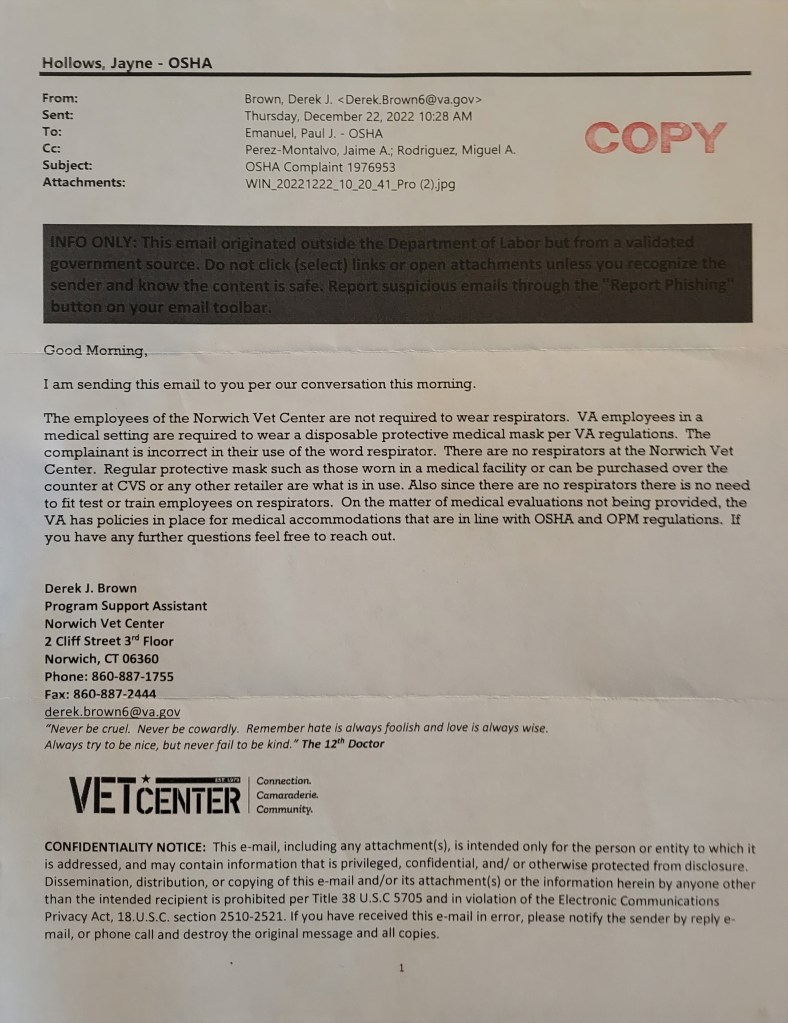
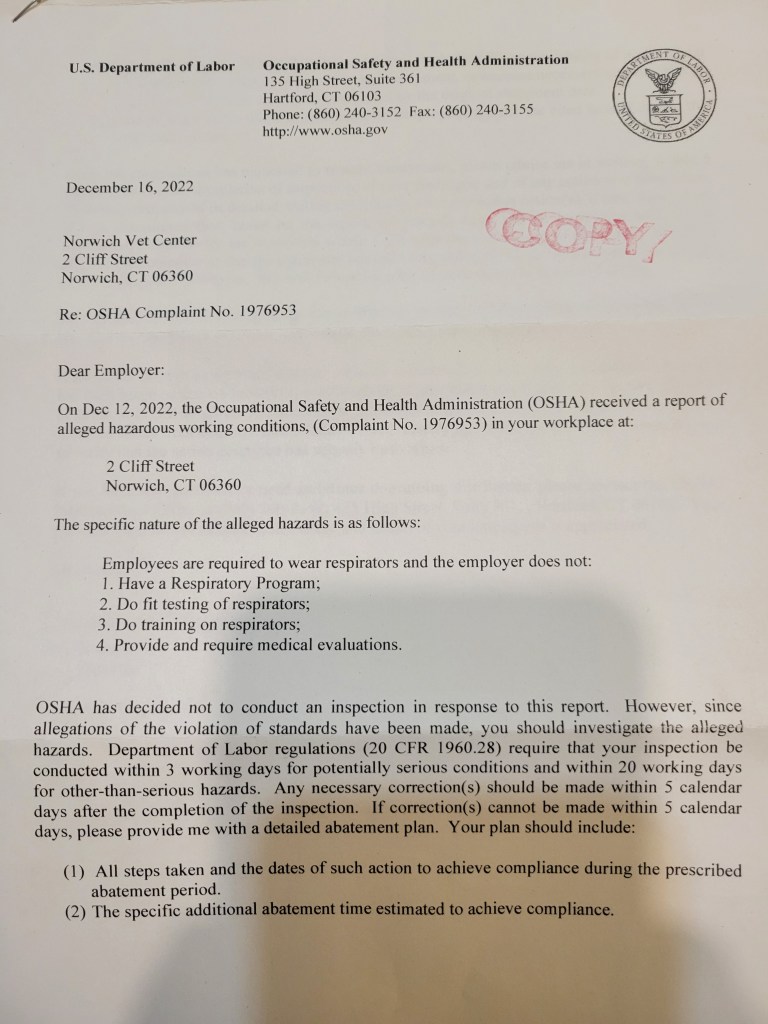
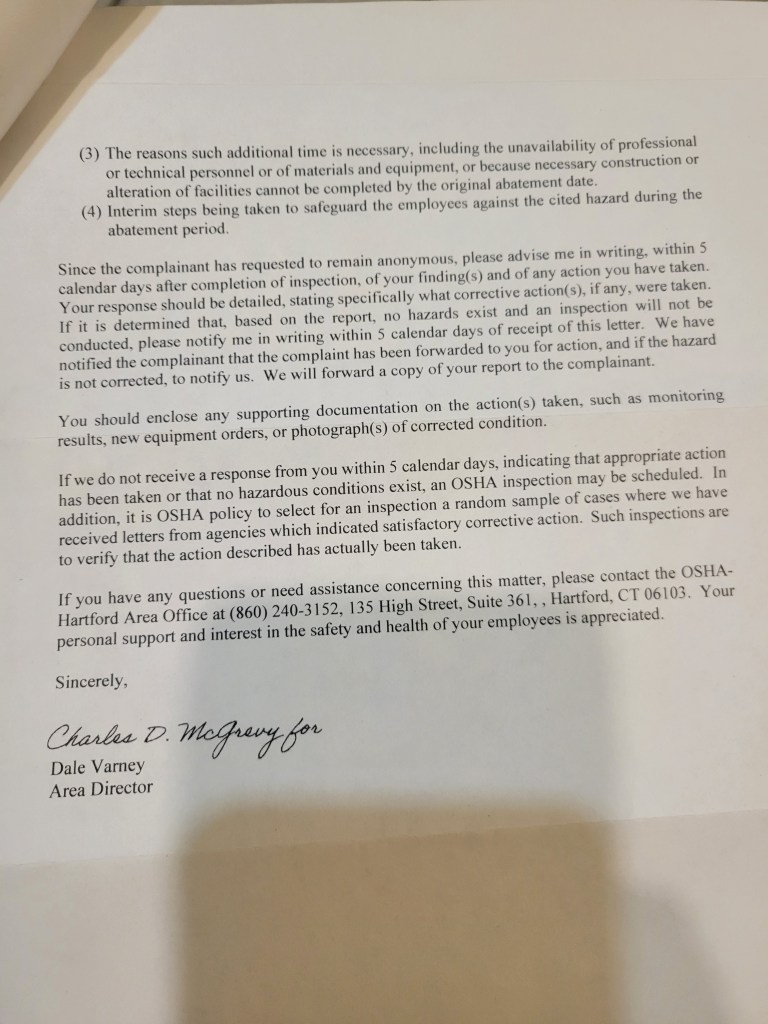
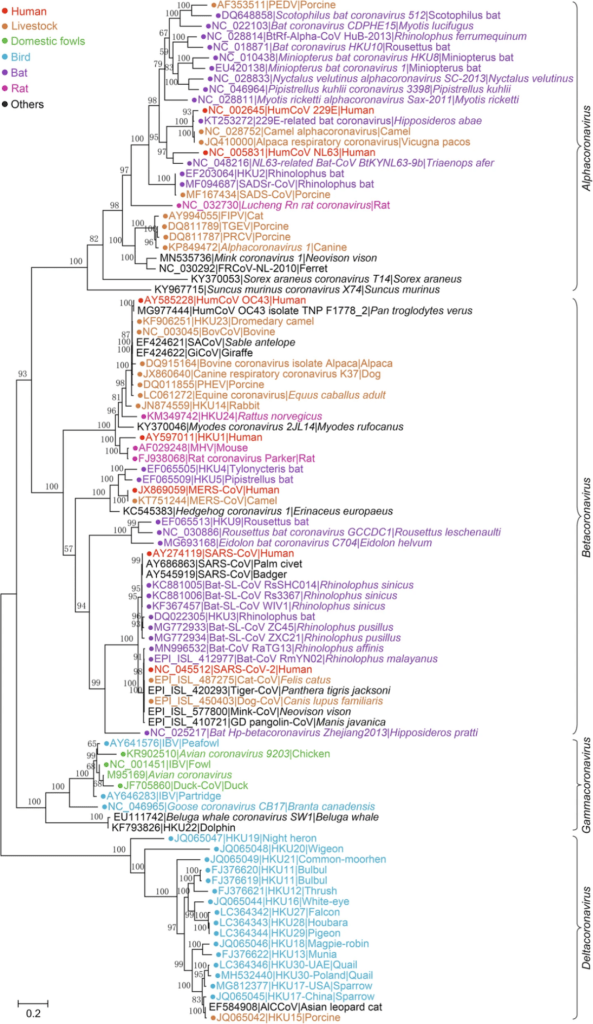

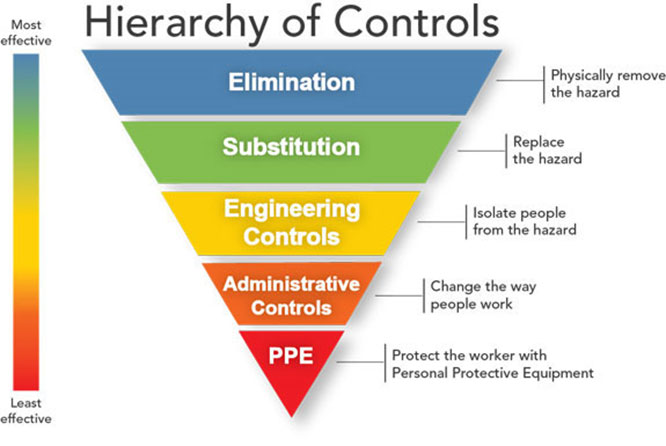
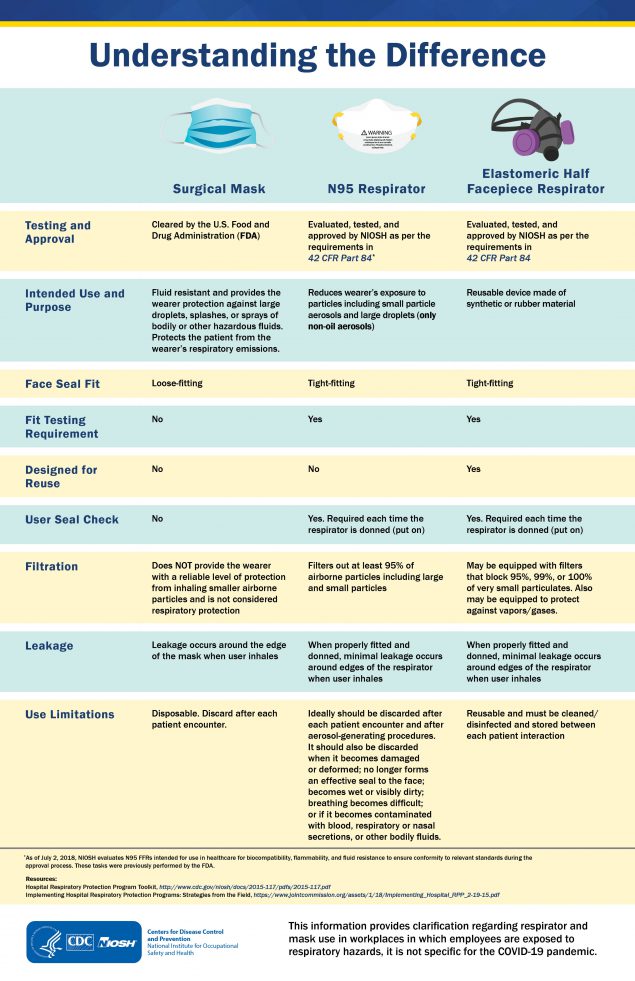


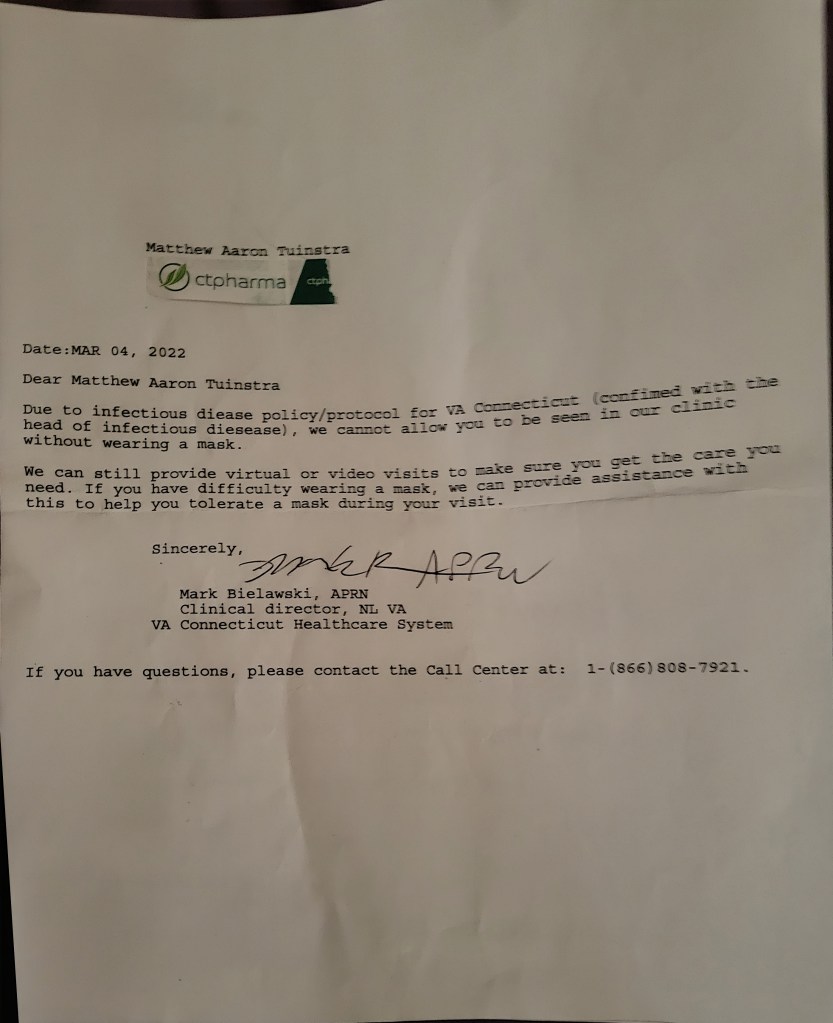

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}